Center for Interdisciplinary Research on Nicotine Addiction, Department of Psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia.
Department of Medicine, University of California, San Francisco.
JAMA Netw Open. 2018 Aug;1(4):e181346. doi: 10.1001/jamanetworkopen.2018.1346. Epub 2018 Aug 24.
The US Food and Drug Administration (FDA) has announced its intention to reduce the nicotine content in combustible cigarettes but must base regulation on public health benefits. Fast nicotine metabolizers may be at risk for increased smoking following a national nicotine reduction policy. We hypothesized that using reduced nicotine content (RNC) cigarettes would be associated with increases in smoking behaviors and exposure among smokers with a fast-but not slow-nicotine-metabolite ratio (NMR).
To examine the association of RNC cigarettes with smoking behaviors and biomarkers of exposure and to compare these associations in fast and slow metabolizers of nicotine based on the NMR.
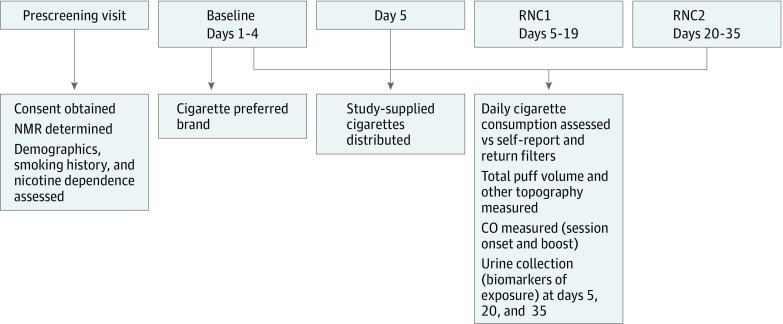
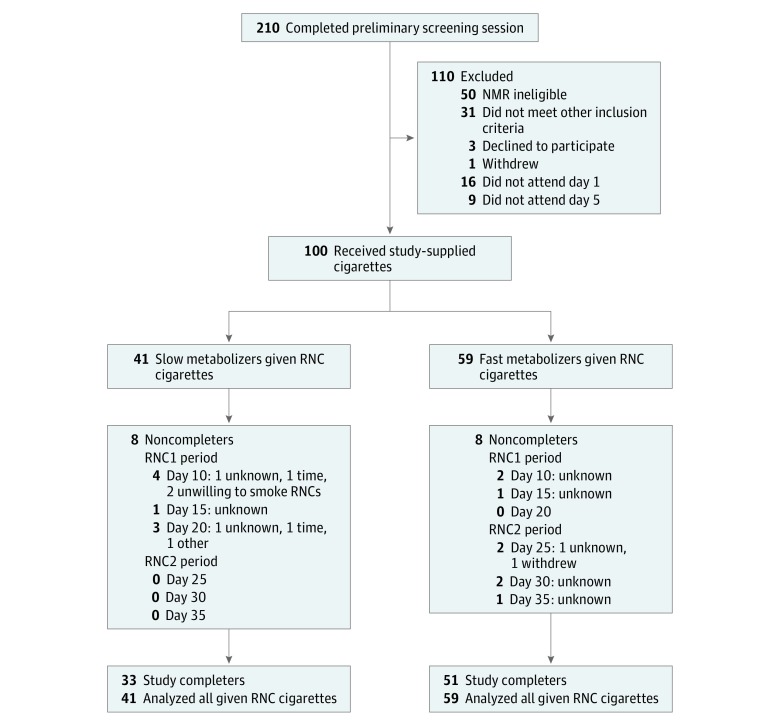
A 35-day, 3-period, within-participant nonrandomized clinical trial was conducted at an academic medical center in Philadelphia, Pennsylvania. A 5-day baseline period using the smokers' preferred brand of cigarettes was followed by 2 consecutive 15-day periods using free investigational RNC cigarettes. A total of 100 daily, non-treatment-seeking, nonmenthol cigarette smokers (59 fast, 41 slow metabolizers) were recruited from December 24, 2013, to December 2, 2015. Data analysis was performed from December 12, 2016, to January 3, 2018.
Two 15-day periods using cigarettes containing 5.2 mg (RNC1) and 1.3 mg (RNC2) of nicotine per gram of tobacco.
Smoking behaviors (number of cigarettes per day [CPD], total puff volume) and biomarkers of exposure (carbon monoxide [CO], urine total nicotine equivalents [TNE], and 4-[methylnitrosamino]-1-[3-pyridyl]-1-butanol [NNAL]).
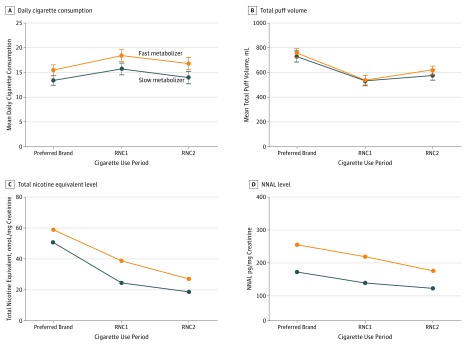
Smokers (73 [73.0%] men; 74 [74.0%] white; mean [SD] age, 43.02 [12.13] years; mean [SD] CPD, 17.31 [5.72]) consumed 2.62 (95% CI, 1.54-3.70) more CPD during the RNC1 period vs their preferred brand during baseline ( < .001) and approximated baseline CPD during the RNC2 period (mean difference, 0.96 [95% CI, -0.36 to 2.28]; = .24). Additional outcome measures were lower during both RNC periods vs baseline (total puff volume, mean [95% CI]: RNC1, 537 mL [95% CI, 479-595 mL]; RNC2, 598 mL [95% CI, 547-649 mL] vs baseline, 744 mL [95% CI, 681-806 mL]; TNE, mean [95% CI]: RNC1, 30.9 nmoL/mg creatinine [95% CI, 26.0-36.6 nmoL/mg]; RNC2, 22.8 nmoL/mg creatinine [95% CI, 17.8-29.0 nmoL/mg] vs baseline, 54.6 nmoL/mg creatinine [95% CI, 48.1-62.1 nmoL/mg]; and NNAL, mean [95% CI]: RNC1, 229 pg/mg creatinine [95% CI, 189-277 pg/mg]; RNC2, 190 pg/mg creatinine [95% CI, 157-231 pg/mg] vs baseline, 280 pg/mg creatinine [95% CI, 231-339 pg/mg]; all < .001). Carbon monoxide measures were similar across study periods (CO boost [SD], RNC1, 4.6 ppm [4.1-5.1 ppm]; RNC2, 4.2 ppm [3.7-4.6 ppm]; and baseline, 4.4 ppm [3.8-4.9 ppm]). The RNC cigarette associations did not differ by NMR.
Both RNC cigarettes were associated with decreased puffing and urinary biomarker exposure but not with decreased daily cigarette consumption or CO levels. The NMR did not moderate associations at the nicotine levels tested, suggesting that fast metabolizers may not be at greater risk of increasing use or exposure from these products should the FDA mandate an RNC standard for cigarettes.
美国食品和药物管理局(FDA)已宣布打算降低可燃香烟中的尼古丁含量,但必须基于公共健康效益来制定监管政策。快速尼古丁代谢者可能会在全国性的尼古丁减少政策出台后增加吸烟量。我们假设使用低尼古丁含量(RNC)香烟会增加快速代谢者而不是慢速尼古丁代谢物比值(NMR)的吸烟者的吸烟行为和暴露水平。
检查 RNC 香烟与吸烟行为和暴露生物标志物的关联,并根据 NMR 比较快速和慢速尼古丁代谢者之间的这些关联。
设计、设置和参与者:在宾夕法尼亚州费城的一所学术医学中心进行了一项为期 35 天、3 期、参与者内非随机临床试验。使用吸烟者喜欢的香烟品牌进行 5 天的基线期,然后连续使用 2 个 15 天的免费 RNC 香烟期。共有 100 名每日非治疗性、非薄荷醇香烟吸烟者(59 名快速代谢者,41 名慢速代谢者)于 2013 年 12 月 24 日至 2015 年 12 月 2 日招募。数据分析于 2016 年 12 月 12 日至 2018 年 1 月 3 日进行。
使用每克烟草含有 5.2 毫克(RNC1)和 1.3 毫克(RNC2)尼古丁的香烟进行 2 个 15 天的试验。
吸烟行为(每天吸烟量[CPD]、总吸烟量)和暴露生物标志物(一氧化碳[CO]、尿总尼古丁当量[TNE]和 4-[甲基亚硝氨基]-1-[3-吡啶基]-1-丁醇[NNAL])。
吸烟者(73 [73.0%] 男性;74 [74.0%] 白人;平均[SD]年龄 43.02 [12.13] 岁;平均[SD]CPD 17.31 [5.72])在 RNC1 期比基线期(<.001)多消耗 2.62(95%CI,1.54-3.70)支 CPD,并且在 RNC2 期接近基线 CPD(平均差异,0.96 [95%CI,-0.36 至 2.28]; =.24)。其他结果指标在两个 RNC 期都低于基线(总吸烟量,平均值[95%CI]:RNC1,537 毫升[95%CI,479-595 毫升];RNC2,598 毫升[95%CI,547-649 毫升]比基线,744 毫升[95%CI,681-806 毫升];TNE,平均值[95%CI]:RNC1,30.9 nmol/mg 肌酐[95%CI,26.0-36.6 nmol/mg];RNC2,22.8 nmol/mg 肌酐[95%CI,17.8-29.0 nmol/mg]比基线,54.6 nmol/mg 肌酐[95%CI,48.1-62.1 nmol/mg];NNAL,平均值[95%CI]:RNC1,229 pg/mg 肌酐[95%CI,189-277 pg/mg];RNC2,190 pg/mg 肌酐[95%CI,157-231 pg/mg]比基线,280 pg/mg 肌酐[95%CI,231-339 pg/mg];所有结果均<.001)。研究期间 CO 测量值相似(CO 提升[SD],RNC1,4.6 ppm [3.7-5.1 ppm];RNC2,4.2 ppm [3.7-4.6 ppm];和基线,4.4 ppm [3.8-4.9 ppm])。RNC 香烟的关联与吸烟行为和尿液生物标志物暴露的降低有关,但与每日吸烟量或 CO 水平的降低无关。在测试的尼古丁水平下,NMR 没有调节关联,这表明在 FDA 强制实施香烟低尼古丁含量标准的情况下,快速代谢者可能不会增加使用或暴露于这些产品的风险。