Division of Pulmonary and Critical Care Medicine, Dept of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea.
These two authors contributed equally to this work.
Eur Respir J. 2019 Mar 18;53(3). doi: 10.1183/13993003.01508-2018. Print 2019 Mar.
Guidelines recommend invasive mediastinal staging for centrally located tumours, even in radiological N0 nonsmall cell lung cancer (NSCLC). However, there is no uniform definition of a central tumour that is more predictive of occult mediastinal metastasis.
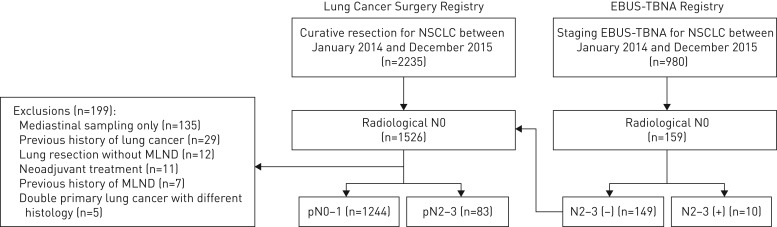
A total of 1337 consecutive patients with radiological N0 disease underwent invasive mediastinal staging. Tumours were categorised into central and peripheral by seven different definitions.
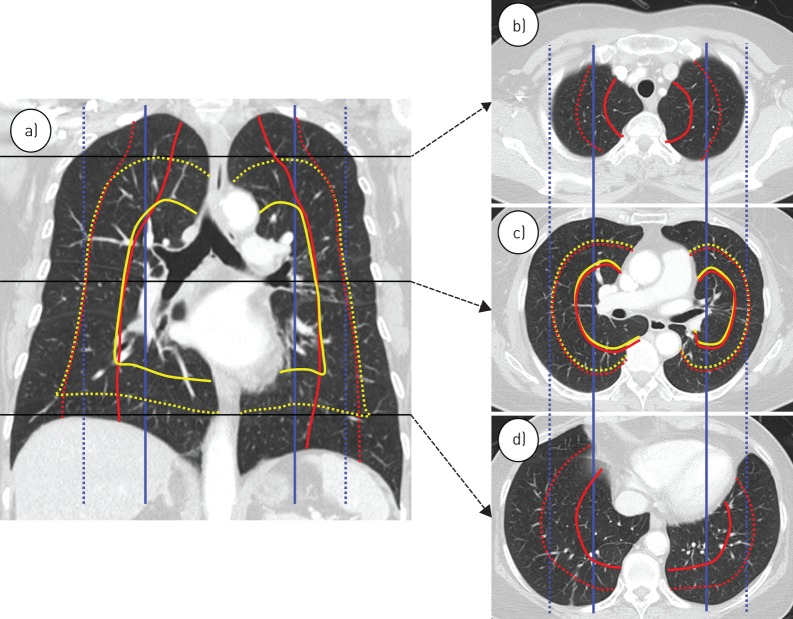
About 7% (93 out of 1337) of patients had occult N2 disease, and they had significantly larger tumour size and more solid tumours on computed tomography. After adjustment for patient- and tumour-related characteristics, only the central tumour definition of the inner one-third of the hemithorax adopted by drawing concentric lines arising from the midline significantly predicted occult N2 disease (adjusted OR 2.13, 95% CI 1.17-3.87; p=0.013). This association was maintained after excluding patients with pure ground-glass nodules (adjusted OR 2.54, 95% CI 1.37-4.71; p=0.003) or only including those with solid tumours (adjusted OR 2.30, 95% CI 1.08-4.88; p=0.030).
We suggest that a central tumour should be defined using the inner one-third of the hemithorax adopted by drawing concentric lines from the midline. This is particularly useful for predicting occult N2 disease in patients with NSCLC.
指南建议对中央型肿瘤进行有创性纵隔分期,即使在影像学 N0 非小细胞肺癌(NSCLC)中也是如此。然而,对于更能预测隐匿性纵隔转移的中央型肿瘤,目前尚无统一的定义。
共对 1337 例影像学 N0 疾病的连续患者进行了有创性纵隔分期。肿瘤通过七种不同的定义分为中央型和周围型。
约 7%(93/1337)的患者存在隐匿性 N2 疾病,且其肿瘤体积更大,CT 上实性肿瘤更多。在调整了患者和肿瘤相关特征后,仅从中线引出的同心线将胸腔的内三分之一作为中央型肿瘤定义,能显著预测隐匿性 N2 疾病(调整后的 OR 2.13,95%CI 1.17-3.87;p=0.013)。在排除了纯磨玻璃结节(调整后的 OR 2.54,95%CI 1.37-4.71;p=0.003)或仅包括实性肿瘤的患者(调整后的 OR 2.30,95%CI 1.08-4.88;p=0.030)后,这种相关性仍然存在。
我们建议采用从中线引出的同心线将胸腔的内三分之一作为中央型肿瘤的定义。这对于预测 NSCLC 患者隐匿性 N2 疾病特别有用。