1 Division of Cardiology IRCCS Fondazione Policlinico S. Matteo Pavia Italy.
2 First Division of Cardiology Ospedale Niguarda Milano Italy.
J Am Heart Assoc. 2019 Jan 22;8(2):e010956. doi: 10.1161/JAHA.118.010956.
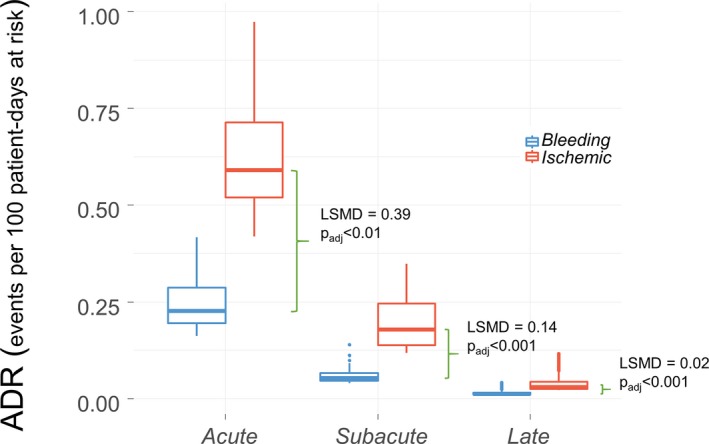
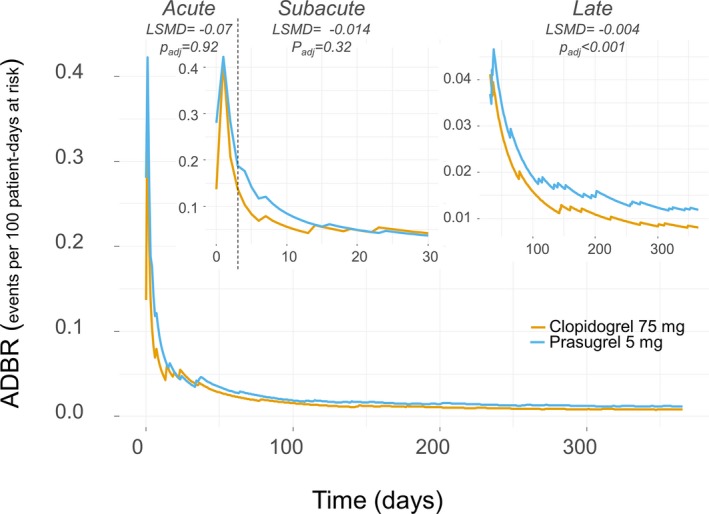
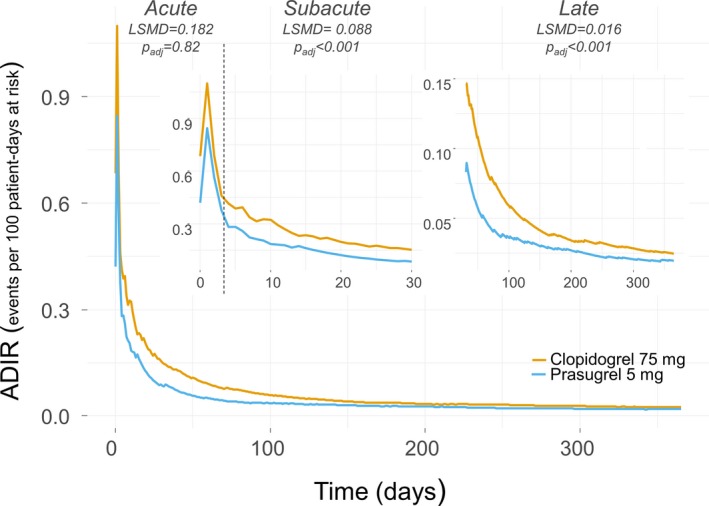
Background Elderly patients have high ischemic and bleeding rates after acute coronary syndrome; however, the occurrence of these complications over time has never been studied. This study sought to characterize average daily ischemic rates ( ADIRs ) and average daily bleeding rates ( ADBRs ) over 1 year in patients aged >74 years with acute coronary syndrome undergoing percutaneous coronary intervention who were randomized in the Elderly ACS 2 trial, comparing low-dose prasugrel (5 mg daily) with clopidogrel (75 mg daily). Methods and Results ADIRs and ADBRs were calculated as the total number of events, including recurrent events, divided by the number of patient-days of follow-up and assessed within different clinical phases: acute (0-3 days), subacute (4-30 days), and late (31-365 days). Generalized estimating equations were used to test the least squares mean differences for the pairwise comparisons of ADIRs and ADBRs and the pairwise comparison of clopidogrel versus prasugrel effects. Globally, ADIRs were 2.6 times (95% CI, 2.4-2.9) higher than ADBRs . ADIRs were significantly higher in the clopidogrel arm than in the low-dose prasugrel arm in the subacute phase ( P<0.001) without a difference in ADBRs ( P=0.35). In the late phase, ADIRs remained significantly higher with clopidogrel ( P<0.001), whereas ADBRs were significantly higher with low-dose prasugrel ( P<0.001). Conclusions Ischemic burden was greater than bleeding burden in all clinical phases of 1-year follow-up of elderly patients with acute coronary syndrome treated with percutaneous coronary intervention. Low-dose prasugrel reduced ischemic events in the subacute and chronic phases compared with clopidogrel, whereas bleeding burden was lower with clopidogrel in the late phase. Clinical Trial Registration URL : http://www.clinicaltrials.gov . Unique identifier: NCT 01777503.
老年急性冠状动脉综合征(acute coronary syndrome,ACS)患者发生缺血和出血的风险较高;然而,这些并发症随时间的发生情况从未被研究过。本研究旨在描述接受经皮冠状动脉介入治疗的老年 ACS 患者(年龄>74 岁)在 1 年期间平均每日缺血率(average daily ischemic rates,ADIRs)和平均每日出血率(average daily bleeding rates,ADBRs)的变化,该研究是 Elderly ACS 2 试验的一部分,比较了低剂量普拉格雷(每天 5mg)与氯吡格雷(每天 75mg)的疗效。
ADIRs 和 ADBRs 是通过将总事件数(包括复发性事件)除以随访患者天数计算得出的,并在不同的临床阶段进行评估:急性期(0-3 天)、亚急性期(4-30 天)和晚期(31-365 天)。采用广义估计方程比较 ADIRs 和 ADBRs 的最小二乘均数差异,并比较氯吡格雷与普拉格雷的疗效。总体而言,ADIRs 是 ADBRs 的 2.6 倍(95%置信区间,2.4-2.9)。在亚急性期,氯吡格雷组的 ADIRs 显著高于低剂量普拉格雷组(P<0.001),而两组的 ADBRs 无差异(P=0.35)。在晚期,氯吡格雷组的 ADIRs 仍显著升高(P<0.001),而低剂量普拉格雷组的 ADBRs 显著升高(P<0.001)。
在接受经皮冠状动脉介入治疗的老年急性冠状动脉综合征患者 1 年随访的所有临床阶段,缺血负担均大于出血负担。与氯吡格雷相比,低剂量普拉格雷在亚急性期和慢性期减少了缺血事件,而氯吡格雷在晚期出血负担较低。
http://www.clinicaltrials.gov。唯一标识符:NCT 01777503。