Department of Cardiology, Keio University School of Medicine, Tokyo, Japan.
Division of Cardiovascular Medicine, Department of Medicine, Stanford University, Stanford, California.
JAMA Netw Open. 2020 Apr 1;3(4):e202004. doi: 10.1001/jamanetworkopen.2020.2004.
Prasugrel was approved at a lower dose in 2014 in Japan than in the West because East Asian patients are considered more susceptible to bleeding than Western patients. However, real-world outcomes with low-dose prasugrel treatment remain unclear.
To investigate the association of low-dose prasugrel vs standard-dose clopidogrel administration with short-term outcomes among patients with acute coronary syndrome undergoing percutaneous coronary intervention (PCI).
DESIGN, SETTING, AND PARTICIPANTS: This study used data from the Japan Cardiovascular Database-Keio Interhospital Cardiovascular Studies registry, a large, ongoing, multicenter, retrospective cohort of consecutive patients who underwent PCI. The present cohort study evaluated 2770 patients with acute coronary syndrome who underwent PCI and received either low-dose prasugrel (loading dose, 20 mg; maintenance dose, 3.75 mg) or clopidogrel (loading dose, 300 mg; maintenance dose, 75 mg) in combination with aspirin between 2014 and 2018. Propensity score-matching analysis was conducted to balance the baseline characteristics of patients receiving low-dose prasugrel and those receiving clopidogrel. Data analysis was conducted in June 2019.
Prescription of either low-dose prasugrel or standard-dose clopidogrel prior to PCI.
Primary ischemic events (in-hospital death, recurrent myocardial infarction, and ischemic stroke) and primary bleeding events, defined as bleeding complications within 72 hours after PCI consistent with the National Cardiovascular Data Registry CathPCI Registry definition.
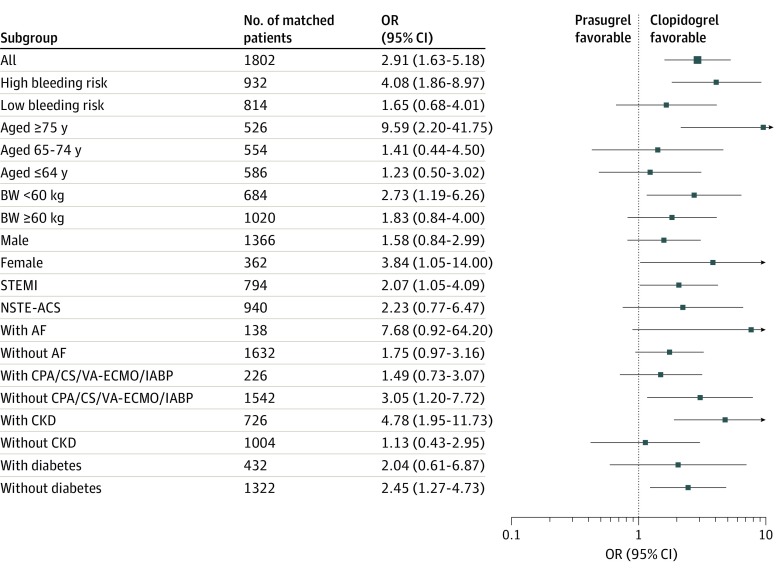
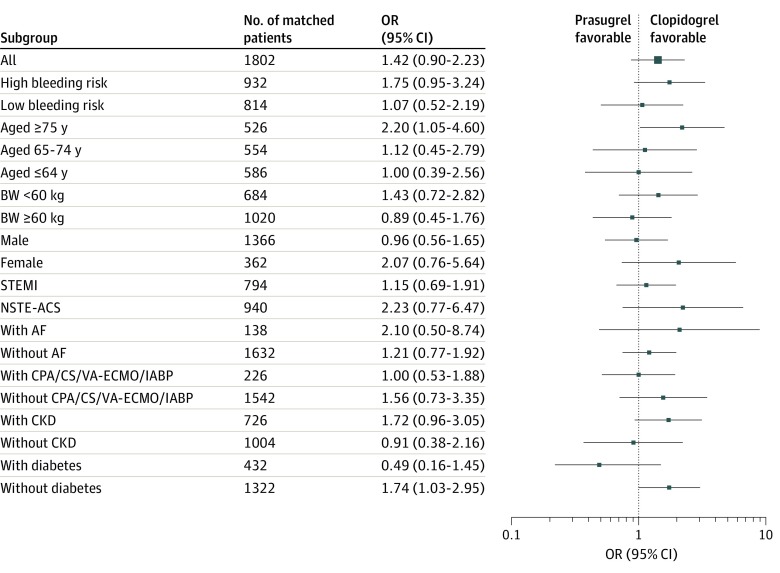
Of 2559 patients included in the study, the mean (SD) age was 67.8 (12.7) years, and 78.2% were male. In total, 1297 patients (50.7%) received low-dose prasugrel, and 1262 patients (49.3%) received clopidogrel. After propensity score matching, primary ischemic events among patients receiving low-dose prasugrel and those receiving clopidogrel were comparable (odds ratio [OR], 1.42; 95% CI, 0.90-2.23), but primary bleeding events were significantly higher among patients receiving prasugrel (OR, 2.91; 95% CI, 1.63-5.18). This increase in bleeding events was associated with the presence of a profile of high-bleeding risk (≥75 years of age, body weight <60 kg, or history of stroke or transient ischemic attack) (OR, 4.08; 95% CI, 1.86-8.97), being female (OR, 3.84; 95% CI, 1.05-14.0), or the presence of ST-segment elevation myocardial infarction (OR, 2.07; 95% CI, 1.05-4.09) or chronic kidney disease (OR, 4.78; 95% CI, 1.95-11.7).
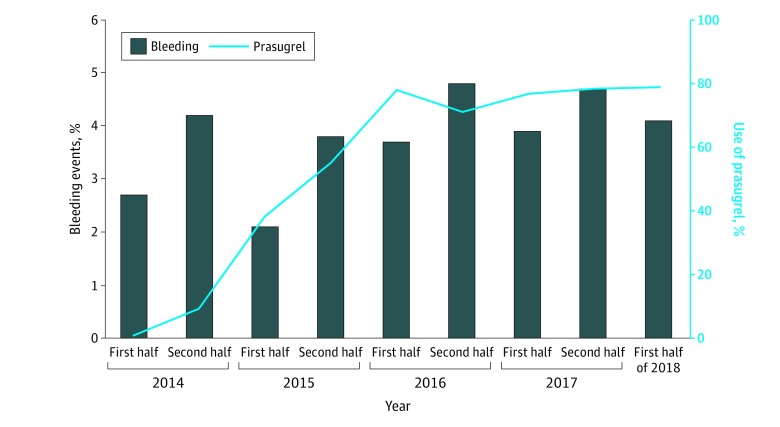
Since its approval, low-dose prasugrel has been used by nearly 80% of patients who undergo PCI. Despite the modified dose, bleeding events were higher among patients receiving low-dose prasugrel than among patients receiving clopidogrel, with no difference in ischemic events between the 2 groups. These results suggest the importance of a risk assessment of bleeding prior to selecting a P2Y12 inhibitor, even for the use of a lower approved dose, when treating patients of East Asian descent.
重要性:2014 年,比伐卢定在日本的批准剂量低于西方,因为东亚患者被认为比西方患者更容易出血。然而,低剂量比伐卢定治疗的真实世界结果仍不清楚。
目的:研究急性冠状动脉综合征行经皮冠状动脉介入治疗(PCI)的患者中,低剂量比伐卢定与标准剂量氯吡格雷给药与短期结局的相关性。
设计、地点和参与者:本研究使用了日本心血管数据库-庆应义塾大学医院心血管研究注册中心的数据,这是一个正在进行的、多中心、回顾性的连续患者队列研究,这些患者接受了 PCI。本队列研究评估了 2014 年至 2018 年间接受 PCI 并接受低剂量比伐卢定(负荷剂量 20mg;维持剂量 3.75mg)或氯吡格雷(负荷剂量 300mg;维持剂量 75mg)联合阿司匹林治疗的 2770 例急性冠状动脉综合征患者。进行了倾向评分匹配分析,以平衡接受低剂量比伐卢定和接受氯吡格雷治疗的患者的基线特征。数据分析于 2019 年 6 月进行。
暴露:PCI 前接受低剂量比伐卢定或标准剂量氯吡格雷的处方。
主要结局和测量:主要缺血事件(住院死亡、复发性心肌梗死和缺血性卒中)和主要出血事件,定义为 PCI 后 72 小时内与国家心血管数据注册 CathPCI 注册中心定义一致的出血并发症。
结果:在纳入的 2559 例患者中,平均(SD)年龄为 67.8(12.7)岁,78.2%为男性。共有 1297 例(50.7%)患者接受低剂量比伐卢定,1262 例(49.3%)患者接受氯吡格雷。经倾向评分匹配后,接受低剂量比伐卢定和氯吡格雷治疗的患者主要缺血事件相当(比值比 [OR],1.42;95%CI,0.90-2.23),但接受比伐卢定治疗的患者主要出血事件显著更高(OR,2.91;95%CI,1.63-5.18)。这种出血事件的增加与高出血风险特征(≥75 岁、体重<60kg 或有卒中或短暂性脑缺血发作史)(OR,4.08;95%CI,1.86-8.97)、女性(OR,3.84;95%CI,1.05-14.0)或 ST 段抬高型心肌梗死(OR,2.07;95%CI,1.05-4.09)或慢性肾脏病(OR,4.78;95%CI,1.95-11.7)有关。
结论和相关性:自批准以来,近 80%接受 PCI 的患者使用了低剂量比伐卢定。尽管剂量有所调整,但与接受氯吡格雷治疗的患者相比,接受低剂量比伐卢定的患者出血事件更多,但两组之间的缺血事件无差异。这些结果表明,即使对于较低的批准剂量,在选择 P2Y12 抑制剂治疗东亚裔患者时,在选择之前进行出血风险评估非常重要。