Department of Medicine and Clinical Science, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan.
Department of Health Care Administration and Management, Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan.
JAMA Netw Open. 2018 Sep 7;1(5):e182953. doi: 10.1001/jamanetworkopen.2018.2953.
It is unknown whether poststroke outcome varies between different potential causes in patients with cryptogenic stroke.
To investigate whether functional outcome differs according to potential embolic sources after cryptogenic stroke.
DESIGN, SETTING, AND PARTICIPANTS: This multicenter, hospital-based, prospective stroke registry cohort study investigated potential embolic sources on admission and assessed 3-month outcome in patients with ischemic stroke hospitalized at 7 stroke centers in the Fukuoka Stroke Registry. This registry enlisted 9866 consecutive patients with acute ischemic stroke who were enrolled from June 11, 2007, to May 31, 2016, in Fukuoka, Japan. Patients with small vessel occlusion (n = 3130), extracranial and intracranial atherosclerosis causing at least 50% luminal stenosis in arteries supplying the area of ischemia (n = 2011), and other specific uncommon causes of stroke identified (n = 301) were excluded. Potential embolic sources were diagnosed in patients with embolic stroke of undetermined source (ESUS) based on the following criteria proposed by the Cryptogenic Stroke/ESUS International Working Group: minor-risk potential cardioembolic sources (MCS) (n = 209), covert paroxysmal atrial fibrillation (CPAF) (n = 43), cancer associated (CA) (n = 79), arteriogenic emboli (AE) (n = 522), paradoxical embolism (PE) (n = 190), and undetermined embolism (unidentified or ≥2 potential embolic sources) (UE) (n = 1120).
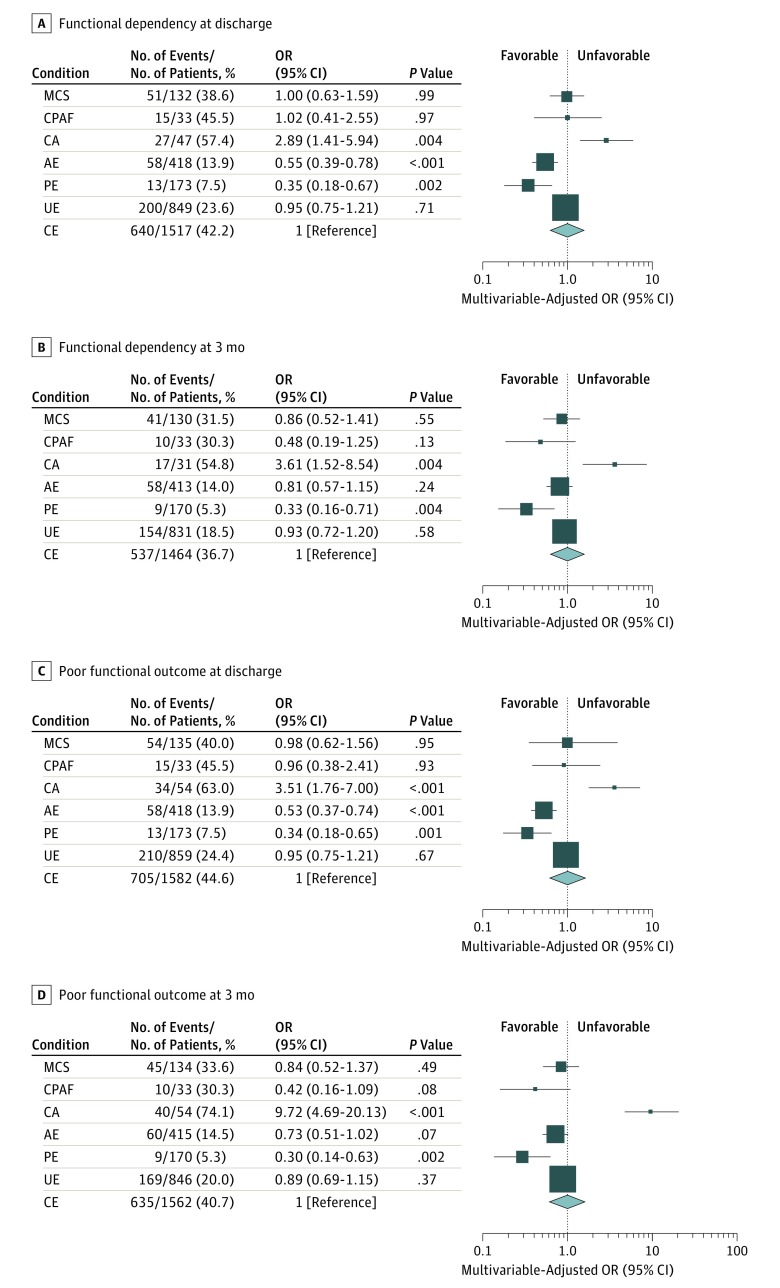
The association between potential causes and functional outcome was evaluated in reference to cardioembolic stroke (CE) caused by major-risk cardioembolic sources after adjusting for age, sex, National Institutes of Health Stroke Scale score on admission, and reperfusion therapy using logistic regression analysis. Functional dependency (modified Rankin Scale score, 3-5) was evaluated at 3 months after onset.
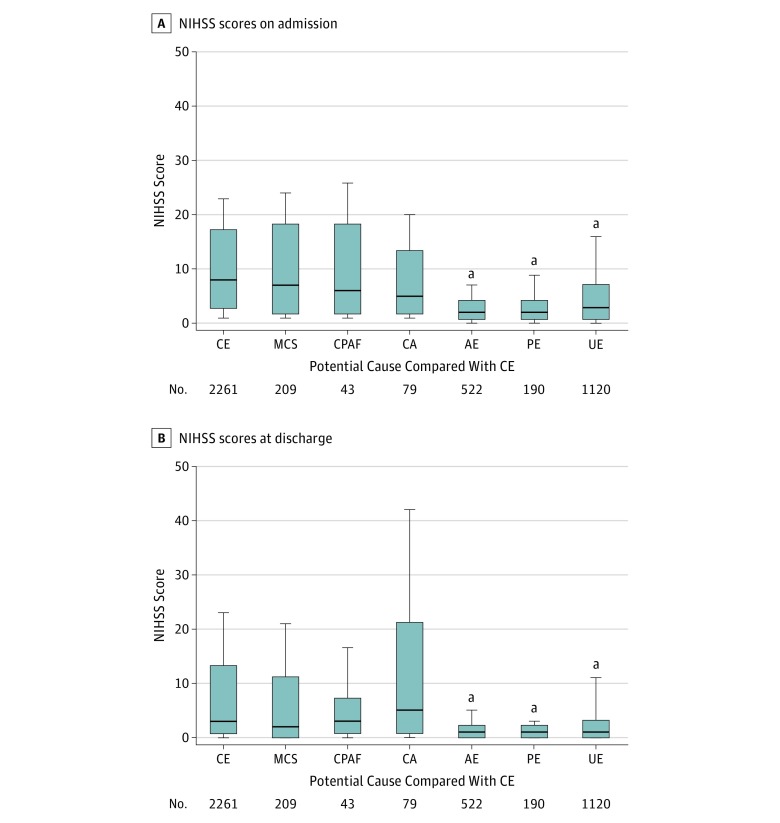
The study enrolled 2261 patients with CE (mean [SD] age, 78.4 [10.7] years, 51.8% male) and 2163 patients with ESUS (mean [SD] age, 72.4 [12.6] years, 57.1% male). Compared with CE (median National Institutes of Health Stroke Scale score, 8 [interquartile range {IQR}, 3-17]), baseline neurological deficits did not differ in MCS (median, 7 [IQR, 2-18]), CPAF (median, 6 [IQR, 2-18]), and CA (median, 5 [IQR, 2-13]) but were less severe in AE (median, 2 [IQR, 1-4]), PE (median, 2 [IQR, 1-4]), and UE (median, 3 [IQR, 1-7]). Multivariable-adjusted odds ratios of functional dependency significantly increased in CA (3.61; 95% CI, 1.52-8.54 vs CE) but decreased in PE (0.33; 95% CI, 0.16-0.71 vs CE).
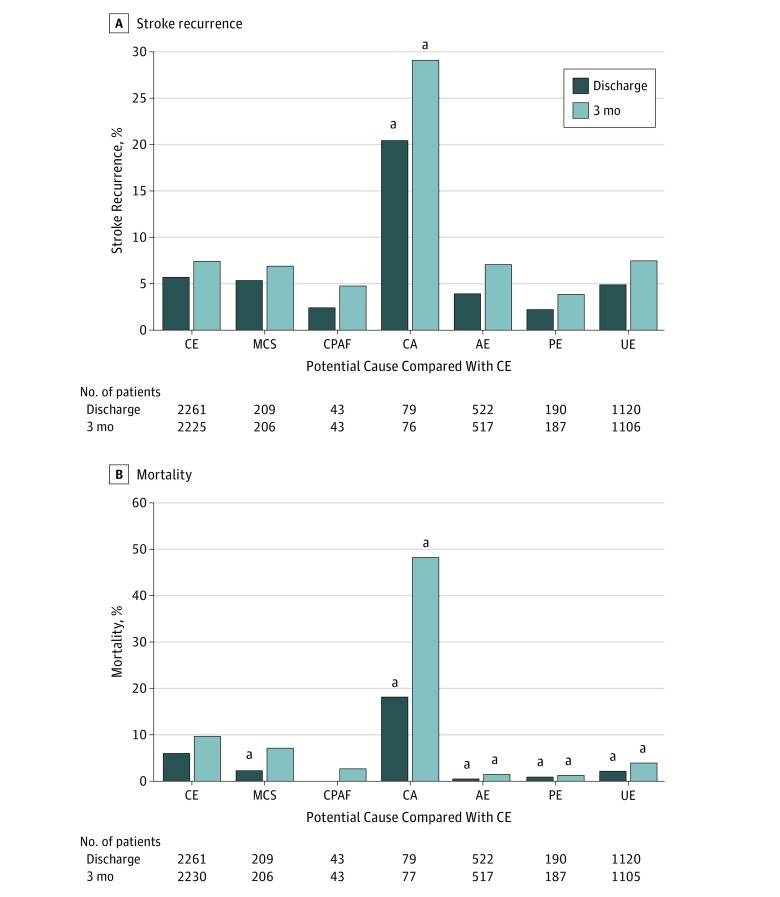
Potential causes are associated with poststroke outcome in patients with cryptogenic stroke. Embolic sources potentially underlying cryptogenic stroke should be considered significant variables associated with outcome.
尚不清楚隐匿性卒中患者的不同潜在病因与卒中后结局之间是否存在差异。
研究隐匿性卒中患者的潜在栓塞源与功能结局是否存在差异。
设计、地点和参与者:这是一项多中心、基于医院的前瞻性卒中登记队列研究,在福冈卒中登记处的 7 家卒中中心对入院时的潜在栓塞源进行了研究,并评估了缺血性卒中患者的 3 个月结局。该登记处纳入了 9866 例连续急性缺血性卒中患者,他们于 2007 年 6 月 11 日至 2016 年 5 月 31 日在日本福冈登记。排除小血管闭塞(n=3130)、至少 50%的管腔狭窄导致颅内和颅外动脉供应区域缺血的动脉粥样硬化(n=2011)和其他特定少见原因的卒中(n=301)。根据隐源性卒中和 ESUS 国际工作组提出的以下标准,对栓塞性卒中来源不明(ESUS)患者进行潜在栓塞源诊断:低危心源性栓塞源(MCS)(n=209)、隐匿性阵发性房颤(CPAF)(n=43)、癌症相关(CA)(n=79)、动脉源栓子(AE)(n=522)、反常栓塞(PE)(n=190)和不明原因栓塞(不明原因或≥2 个潜在栓塞源)(UE)(n=1120)。
采用逻辑回归分析,在校正年龄、性别、入院时 NIH 卒中量表评分和再灌注治疗后,评估潜在病因与功能结局的相关性。采用改良 Rankin 量表(mRS)(3-5 分)评估发病 3 个月后的功能依赖性。
该研究纳入了 2261 例心源性栓塞(CE)患者(平均[标准差]年龄 78.4[10.7]岁,51.8%为男性)和 2163 例 ESUS 患者(平均[标准差]年龄 72.4[12.6]岁,57.1%为男性)。与 CE 患者(中位数 NIH 卒中量表评分,8[四分位距 {IQR},3-17])相比,MCS(中位数,7[IQR,2-18])、CPAF(中位数,6[IQR,2-18])和 CA(中位数,5[IQR,2-13])患者的基线神经功能缺损无差异,但 AE(中位数,2[IQR,1-4])、PE(中位数,2[IQR,1-4])和 UE(中位数,3[IQR,1-7])患者的神经功能缺损程度较轻。多变量校正后,CA(3.61;95%CI,1.52-8.54)患者的功能依赖性比值比显著升高,但 PE(0.33;95%CI,0.16-0.71)患者的比值比显著降低。
潜在病因与隐匿性卒中患者的卒中后结局相关。潜在的栓塞源可能是隐匿性卒中的重要变量。