Department of Sociology, University of Utah, 390 South 1530 East, Rm 301, Salt Lake City, UT, 84112, USA.
Population Sciences, Huntsman Cancer Institute, University of Utah, 2000 Circle of Hope, Salt Lake City, UT, 84112, USA.
BMC Public Health. 2019 Jan 22;19(1):100. doi: 10.1186/s12889-019-6391-3.
Driver license departments in many US states collect data on individuals' height and weight. These data can be useful to researchers in epidemiological and public health studies. As height and weight on driver license are self-reported, they may be prone to reporting bias. We compare height and weight obtained from driver license records and clinically measured height and weight, as well as body mass index (BMI) values calculated using the two data sources for the same individual.
We linked individual height and weight records obtained from the Driver License Division (DLD) in the Utah Department of Public Safety to clinical records from one of the largest healthcare providers in the state of Utah. We then calculated average differences between height, weight and BMI values separately for women and men in the sample, as well as discrepancies between the two sets of measures by age and BMI category. We examined how well self-reported height and weight from the driver licenses classify individuals into specific BMI categories based on clinical measures. Finally, we used two sets of BMI values to estimate individuals' relative risk of type II diabetes.
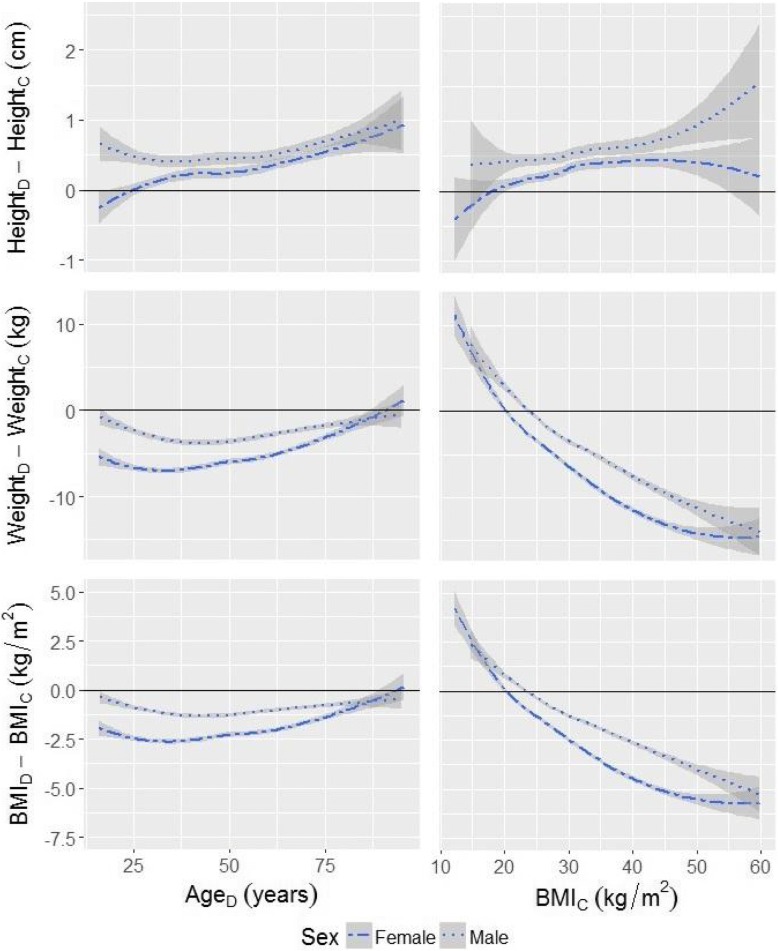
Individuals, on average, tend to overestimate their height and underestimate their weight. Consequently, the value of BMI calculated using driver license records is lower than BMI calculated using clinical measurements. The discrepancy varies by age and by BMI category. Despite the discrepancy, BMI based on self-reported height and weight allows for accurate categorization of individuals at the higher end of the BMI scale, such as the obese. When used as predictors of relative risk of type II diabetes, both sets of BMI values yield similar risk estimates.
Data on height and weight from driver license data can be a useful asset for monitoring population health in states where such information is collected, despite the degree of misreporting associated with self-report.
美国许多州的驾照部门都收集个人身高和体重的数据。这些数据对于流行病学和公共卫生研究的研究人员来说非常有用。由于驾照上的身高和体重是自我报告的,因此可能存在报告偏差。我们比较了从驾照记录中获得的身高和体重以及临床测量的身高和体重,以及使用两个数据源为同一人计算的身体质量指数 (BMI) 值。
我们将从犹他州公共安全部驾照分部 (DLD) 获得的个人身高和体重记录与该州最大的医疗保健提供者之一的临床记录相关联。然后,我们分别计算了样本中女性和男性的身高、体重和 BMI 值的平均差异,以及按年龄和 BMI 类别划分的两套测量值之间的差异。我们检查了从驾照中自我报告的身高和体重如何根据临床测量将个体分类到特定的 BMI 类别中。最后,我们使用两套 BMI 值来估计个体患 II 型糖尿病的相对风险。
个体平均倾向于高估自己的身高,低估自己的体重。因此,使用驾照记录计算的 BMI 值低于使用临床测量计算的值。这种差异因年龄和 BMI 类别而异。尽管存在差异,但基于自我报告的身高和体重的 BMI 仍然可以准确地对 BMI 较高的个体进行分类,例如肥胖者。当用作 II 型糖尿病相对风险的预测因子时,两套 BMI 值都产生了相似的风险估计值。
尽管与自我报告相关的报告偏差程度不同,但从驾照数据中获取的身高和体重数据可以成为监测收集此类信息的州的人口健康的有用资产。