Kim Min Kyoung, Moon Hyoung Yong, Ryu Choon Gun, Kang Hyun, Lee Han Jun, Shin Hwa Yong
Department of Anesthesiology and Pain Medicine, College of Medicine, Chung-Ang University, Seoul, Korea.
Department of Orthopedic Surgery, College of Medicine, Chung-Ang University, Seoul, Korea.
Korean J Pain. 2019 Jan;32(1):30-38. doi: 10.3344/kjp.2019.32.1.30. Epub 2019 Jan 2.
The adductor canal block (ACB) is an effective intervention for postoperative analgesia following total knee arthroplasty (TKA). However, the ideal ACB regimen has not yet been established. We compared the analgesic effects between a continuous ACB group and fentanyl-based intravenous patient-controlled analgesia (IV-PCA) with a single-shot ACB group.
Patients who underwent TKA were randomly allocated to either a continuous ACB group (Group CACB) or IV-PCA with a single-shot ACB group (Group IVACB). Before the surgery, ultrasound guided ACB with 0.5% ropivacaine 20 cc was provided to all patients. Before skin incision, the infusion system (0.2% ropivacaine through an adductor canal catheter in group CACB vs. intravenous fentanyl in group IVACB) was connected. The postoperative pain severity; the side effects of local anesthetics and opioids; administration of rescue analgesics and anti-emetics; and sensorimotor deficits were measured.
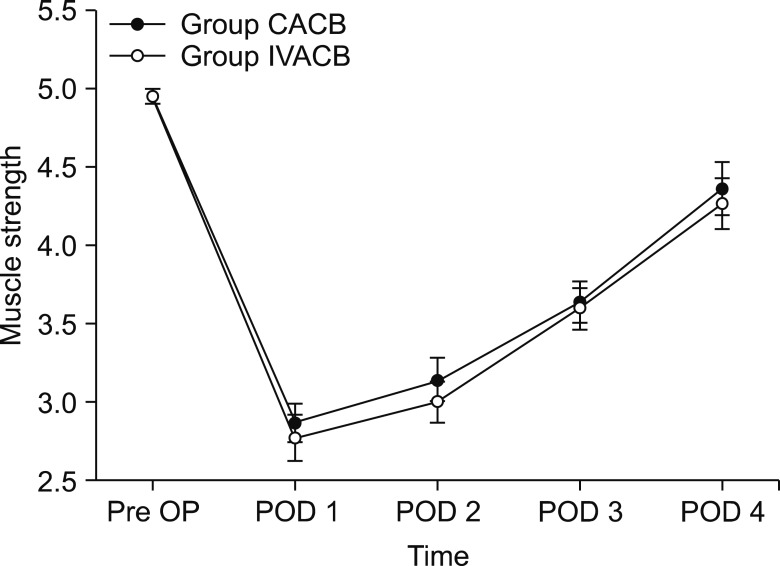
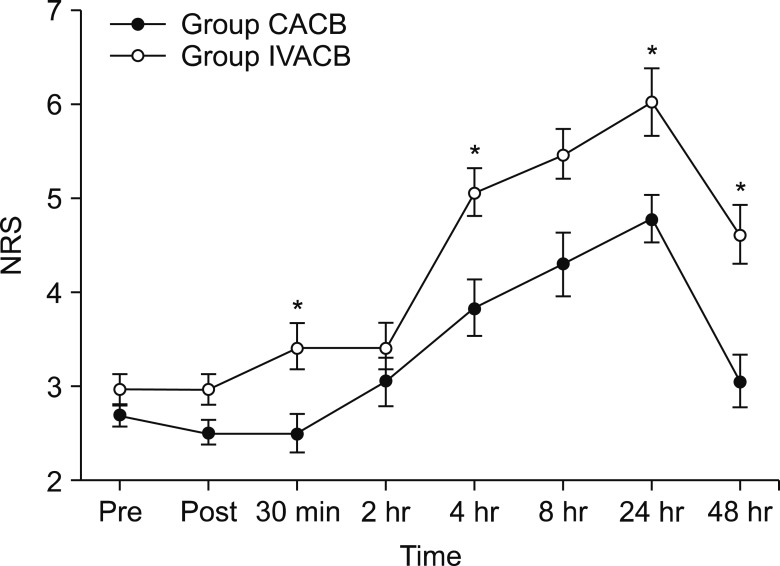
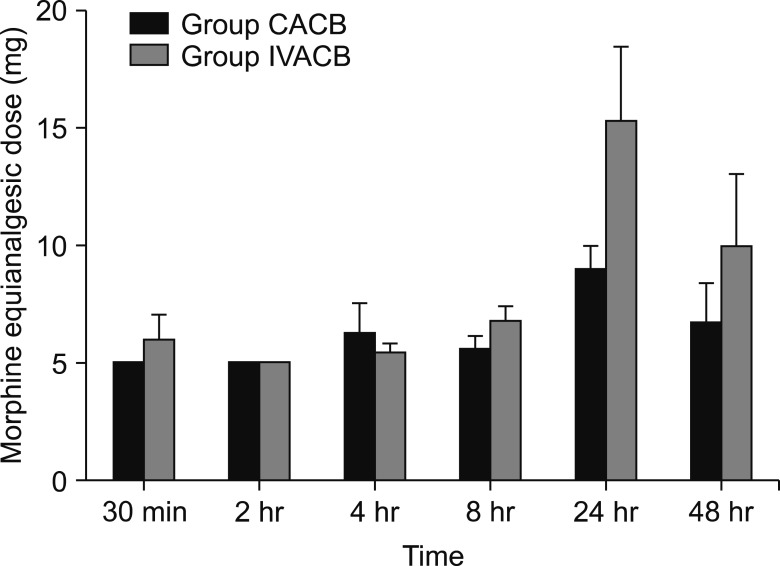
Postoperative pain severity was significantly higher in the IVACB group at 30 min, 4 h, 24 h, and 48 h after surgery. The averages and standard deviations (SD) of the NRS score of postoperative pain were 0.14 ± 0.37, 4.57 ± 2.37, 6.00 ± 1.63, and 4.28 ± 1.49, respectively in the IVACB group. Rescue analgesic requirements and quadriceps muscle strength were not statistically different between the groups throughout the postoperative period. Moreover, rescue antiemetic requirements were higher in group IVACB than group CACB.
In this study, the continuous ACB provided superior analgesia and fewer side effects without any significant motor deficit than the IV-PCA with a single-shot ACB.
收肌管阻滞(ACB)是全膝关节置换术(TKA)后术后镇痛的有效干预措施。然而,理想的ACB方案尚未确立。我们比较了连续ACB组与基于芬太尼的静脉自控镇痛(IV-PCA)联合单次ACB组之间的镇痛效果。
接受TKA的患者被随机分配至连续ACB组(CACB组)或IV-PCA联合单次ACB组(IVACB组)。术前,所有患者均接受超声引导下注射20 cc 0.5%罗哌卡因进行ACB。在皮肤切开前,连接输注系统(CACB组通过收肌管导管输注0.2%罗哌卡因,IVACB组静脉注射芬太尼)。测量术后疼痛严重程度、局部麻醉药和阿片类药物的副作用、急救镇痛药和止吐药的使用情况以及感觉运动功能障碍。
术后30分钟、4小时、24小时和48小时,IVACB组的术后疼痛严重程度显著更高。IVACB组术后疼痛NRS评分的平均值和标准差分别为0.14±0.37、4.57±2.37、6.00±1.63和4.28±1.49。在整个术后期间,两组之间的急救镇痛药需求量和股四头肌力量无统计学差异。此外,IVACB组的急救止吐药需求量高于CACB组。
在本研究中,与IV-PCA联合单次ACB相比,连续ACB提供了更好的镇痛效果,副作用更少,且无明显运动功能障碍。