Sun Changjiao, Zhang Xiaofei, Song Fei, Zhao Zhe, Du Ruiyong, Wu Sha, Ma Qi, Cai Xu
Department of Orthopedic.
Department of Clinical Epidemiology and Biostatistics, Beijing Tsinghua Changgung Hospital, School of Clinical Medicine, Tsinghua University, Beijing, China.
Medicine (Baltimore). 2020 May;99(20):e20320. doi: 10.1097/MD.0000000000020320.
The adductor canal block (ACB) has emerged as an alternative to the femoral nerve block (FNB) after total knee arthroplasty. This meta-analysis was conducted to investigate which ACB method provides better pain relief and functional recovery after total knee arthroplasty METHODS:: We conducted a meta-analysis to identify randomized controlled trials involving single-shot adductor canal block (SACB) and continuous catheter ACB (CACB) after TKA up to December 2019 by searching databases including the PubMed, Web of Science, Embase, Cochrane Controlled Trials Register, Cochrane Library, CBM, CNKI, VIP, and Wanfang databases. Finally, we included 8 randomized controlled trials involving 702 knees in our study. We used Review Manager Software and Grading of Recommendations Assessment, Development, and Evaluation profiler to perform the meta-analysis.
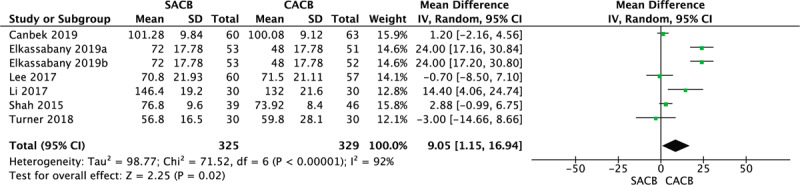
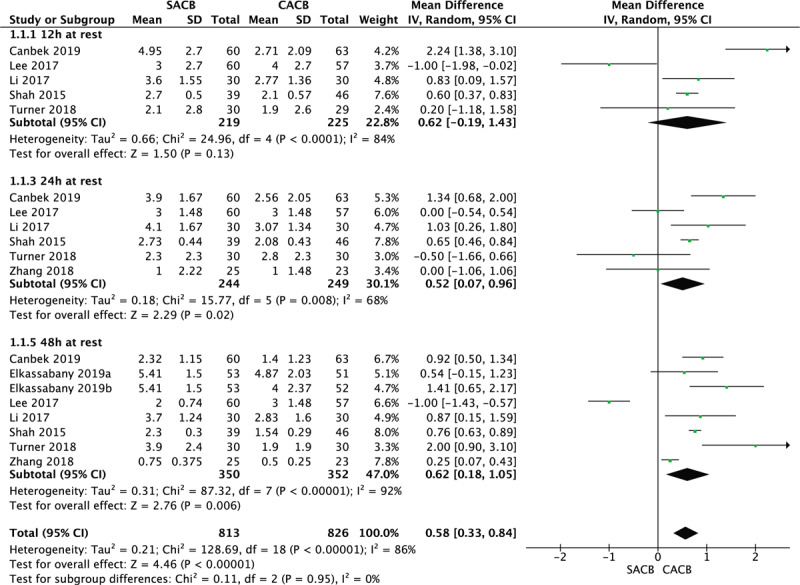
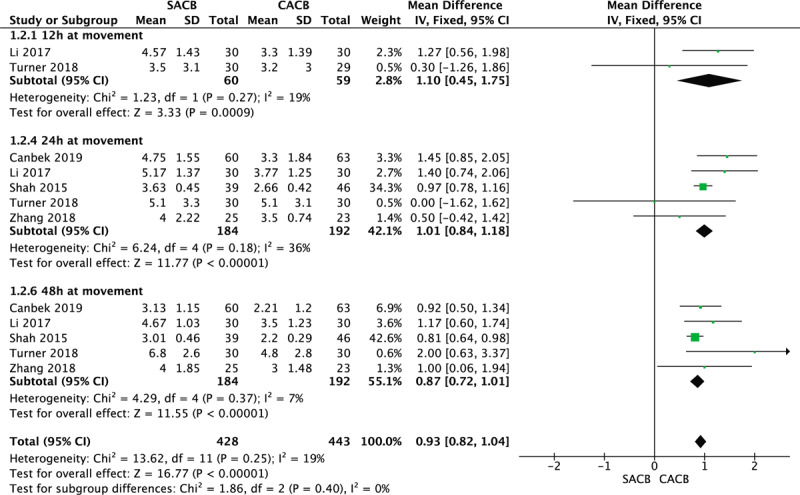
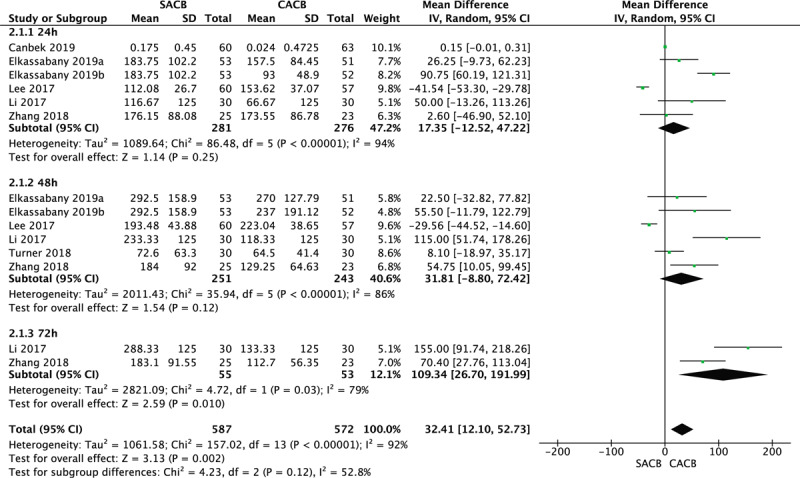
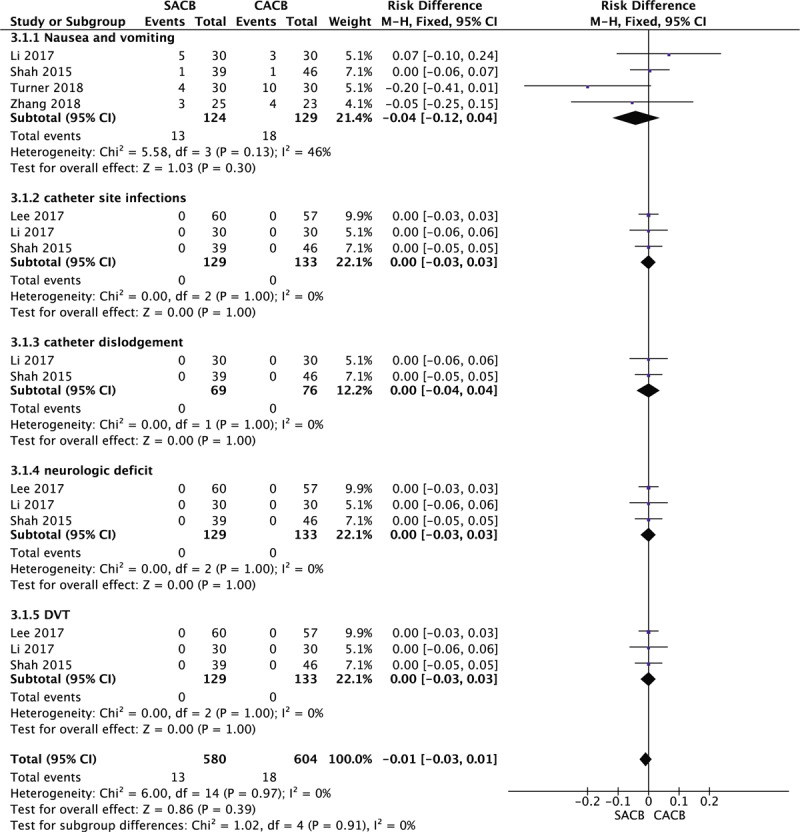
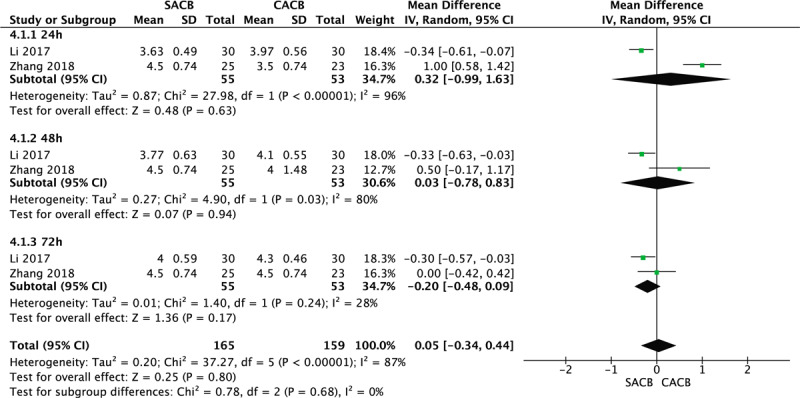
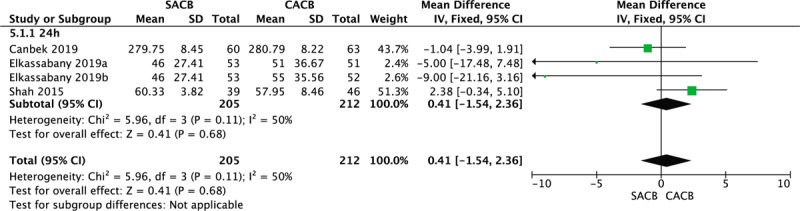
Compared with SACB, CACB can achieve better postoperative pain relief at 24 and 48 h both at rest and after mobilization, lower amount of opioid consumption at 72 h, a shorter length of hospital stay (LOH) and larger range of motion (ROM). In addition, the Timed Up and Go (TUG) test results; quadriceps strength; and incidence of complications, including postoperative nausea and vomiting, DVT, catheter-related infections, catheter dislodgement and neurologic deficits, showed no significant difference between the two ACB methods.
The results of this study demonstrate that CACB is an effective alternative to SACB and can provide better pain relief, a shorter LOH, more degrees of maximum flexion and a lower amount of opioid consumption over time, but it provides a comparable level of recovery of quadriceps strength and mobility with a similar risk of catheter-related complications. Thus, CACB may be a better analgesia strategy than SACB after TKA at present.
收肌管阻滞(ACB)已成为全膝关节置换术后股神经阻滞(FNB)的一种替代方法。本荟萃分析旨在探讨哪种ACB方法能在全膝关节置换术后提供更好的疼痛缓解和功能恢复。
我们通过检索包括PubMed、Web of Science、Embase、Cochrane对照试验注册库、Cochrane图书馆、中国生物医学文献数据库(CBM)、中国知网(CNKI)、维普资讯(VIP)和万方数据库在内的数据库,进行了一项荟萃分析,以确定截至2019年12月的全膝关节置换术(TKA)后单次收肌管阻滞(SACB)和连续导管ACB(CACB)的随机对照试验。最后,我们纳入了8项涉及702个膝关节的随机对照试验进行研究。我们使用Review Manager软件和推荐分级评估、制定与评价工具进行荟萃分析。
与SACB相比,CACB在术后24小时和48小时静息及活动后能实现更好的疼痛缓解,72小时时阿片类药物消耗量更低,住院时间(LOH)更短,活动范围(ROM)更大。此外,定时起立行走(TUG)测试结果、股四头肌力量以及包括术后恶心呕吐、深静脉血栓形成(DVT)、导管相关感染、导管移位和神经功能缺损在内的并发症发生率,在两种ACB方法之间无显著差异。
本研究结果表明,CACB是SACB的一种有效替代方法,随着时间推移,它能提供更好的疼痛缓解、更短的住院时间、更大的最大屈曲度和更低的阿片类药物消耗量,但在股四头肌力量恢复和活动能力方面与SACB相当,且导管相关并发症风险相似。因此,目前在TKA后,CACB可能是比SACB更好的镇痛策略。