Emergency Department, Cabrini Hospital, Malvern, VIC 3144, Australia.
Department of Epidemiology and Preventive Medicine, Monash University, Melbourne, VIC, Australia.
BMJ. 2019 Jan 30;364:l121. doi: 10.1136/bmj.l121.
To evaluate the changes in productivity when scribes were used by emergency physicians in emergency departments in Australia and assess the effect of scribes on throughput.
Randomised, multicentre clinical trial.
Five emergency departments in Victoria used Australian trained scribes during their respective trial periods. Sites were broadly representative of Australian emergency departments: public (urban, tertiary, regional referral, paediatric) and private, not for profit.
88 physicians who were permanent, salaried employees working more than one shift a week and were either emergency consultants or senior registrars in their final year of training; 12 scribes trained at one site and rotated to each study site.
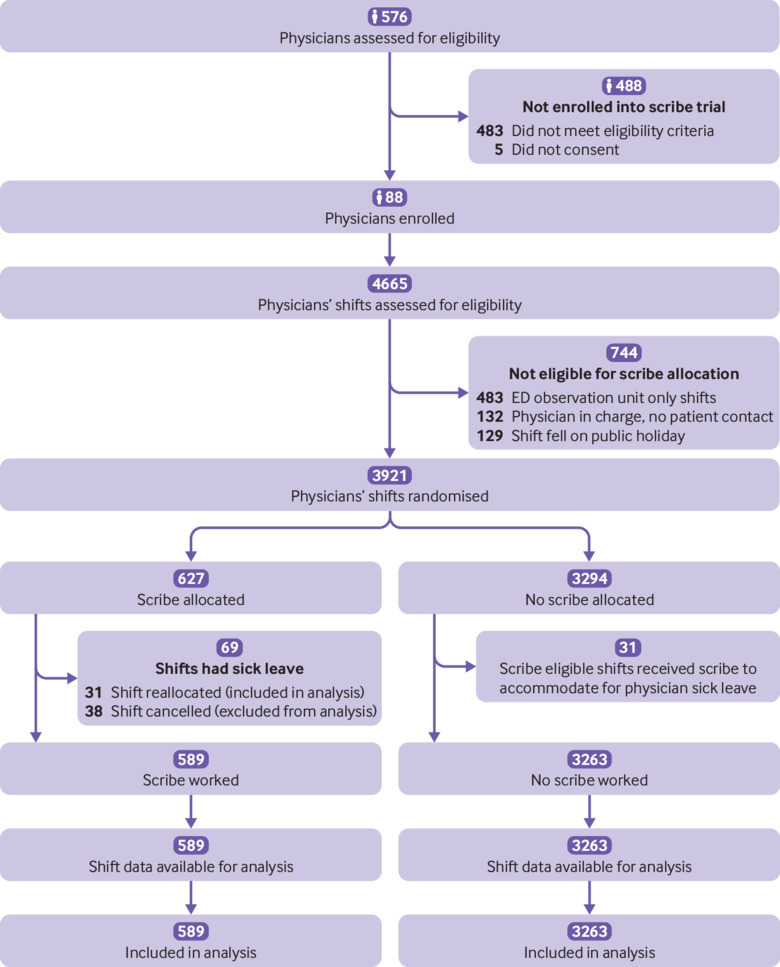
Physicians worked their routine shifts and were randomly allocated a scribe for the duration of their shift. Each site required a minimum of 100 scribed and non-scribed shifts, from November 2015 to January 2018.
Physicians' productivity (total patients, primary patients); patient throughput (door-to-doctor time, length of stay); physicians' productivity in emergency department regions. Self reported harms of scribes were analysed, and a cost-benefit analysis was done.
Data were collected from 589 scribed shifts (5098 patients) and 3296 non-scribed shifts (23 838 patients). Scribes increased physicians' productivity from 1.13 (95% confidence interval 1.11 to 1.17) to 1.31 (1.25 to 1.38) patients per hour per doctor, representing a 15.9% gain. Primary consultations increased from 0.83 (0.81 to 0.85) to 1.04 (0.98 to 1.11) patients per hour per doctor, representing a 25.6% gain. No change was seen in door-to-doctor time. Median length of stay reduced from 192 (interquartile range 108-311) minutes to 173 (96-208) minutes, representing a 19 minute reduction (P<0.001). The greatest gains were achieved by placing scribes with senior doctors at triage, the least by using them in sub-acute/fast track regions. No significant harm involving scribes was reported. The cost-benefit analysis based on productivity and throughput gains showed a favourable financial position with use of scribes.
Scribes improved emergency physicians' productivity, particularly during primary consultations, and decreased patients' length of stay. Further work should evaluate the role of the scribe in countries with health systems similar to Australia's.
ACTRN12615000607572 (pilot site); ACTRN12616000618459.
评估澳大利亚急诊科医生使用抄写员后生产力的变化,并评估抄写员对吞吐量的影响。
随机、多中心临床试验。
维多利亚州的 5 家急诊科在各自的试验期间使用了澳大利亚培训的抄写员。这些地点广泛代表了澳大利亚的急诊科:公立(城市、三级、区域转诊、儿科)和私立非营利。
88 名每周至少工作一个班次的固定、领薪的全职医生,他们是急诊顾问或最后一年培训的高级住院医师;在一个地点接受培训的 12 名抄写员轮流到每个研究地点。
医生按照常规班次工作,并随机分配一名抄写员在整个班次期间协助。从 2015 年 11 月至 2018 年 1 月,每个地点都需要至少 100 次抄写和非抄写班次。
医生的生产力(总患者、主要患者);患者吞吐量(从门口到医生的时间、住院时间);医生在急诊科区域的生产力。分析了抄写员的自我报告伤害,并进行了成本效益分析。
共收集了 589 次抄写(5098 名患者)和 3296 次非抄写(23838 名患者)班次的数据。抄写员使医生的生产力从每小时每医生 1.13(95%置信区间 1.11 至 1.17)增加到 1.31(1.25 至 1.38),增长了 15.9%。主要咨询从每小时每医生 0.83(0.81 至 0.85)增加到 1.04(0.98 至 1.11),增长了 25.6%。从门口到医生的时间没有变化。中位数住院时间从 192(四分位距 108-311)分钟减少到 173(96-208)分钟,减少了 19 分钟(P<0.001)。在分诊时为高级医生配备抄写员的效果最大,在亚急性/快速通道区域使用抄写员的效果最小。没有报告涉及抄写员的任何重大伤害。基于生产力和吞吐量提高的成本效益分析显示使用抄写员具有有利的财务状况。
抄写员提高了急诊医生的生产力,特别是在主要咨询期间,并缩短了患者的住院时间。应进一步评估抄写员在具有类似澳大利亚卫生系统的国家中的作用。
ACTRN12615000607572(试点地点);ACTRN12616000618459。