Department of Internal Medicine III with Hematology, Medical Oncology, Hemostaseology, Infectiology and Rheumatology, Oncologic Center; Salzburg Cancer Research Institute - Laboratory for Immunological and Molecular Cancer Research (SCRI-LIMCR), Paracelsus Medical University, Salzburg, Austria.
Cancer Cluster Salzburg, Salzburg, Austria.
Breast Cancer Res. 2019 Jan 31;21(1):19. doi: 10.1186/s13058-018-1091-y.
Patients with early breast cancer (EBC) achieving pathologic complete response (pCR) after neoadjuvant chemotherapy (NACT) have a favorable prognosis. Breast surgery might be avoided in patients in whom the presence of residual tumor can be ruled out with high confidence. Here, we investigated the diagnostic accuracy of contrast-enhanced MRI (CE-MRI) in predicting pCR and long-term outcome after NACT.
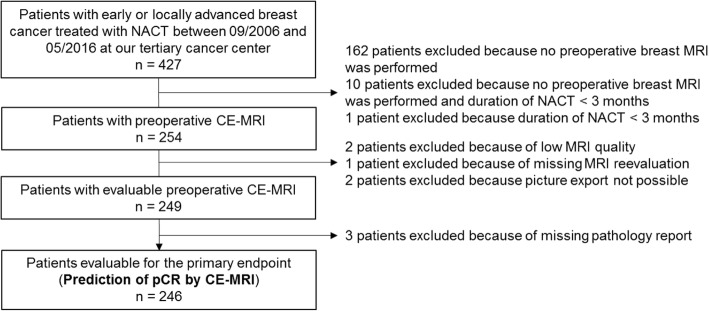
Patients with EBC, including patients with locally advanced disease, who had undergone CE-MRI after NACT, were retrospectively analyzed (n = 246). Three radiologists, blinded to clinicopathologic data, reevaluated all MRI scans regarding to the absence (radiologic complete remission; rCR) or presence (no-rCR) of residual contrast enhancement. Clinical and pathologic responses were compared categorically using Cohen's kappa statistic. The Kaplan-Meier method was used to estimate recurrence-free survival (RFS) and overall survival (OS).
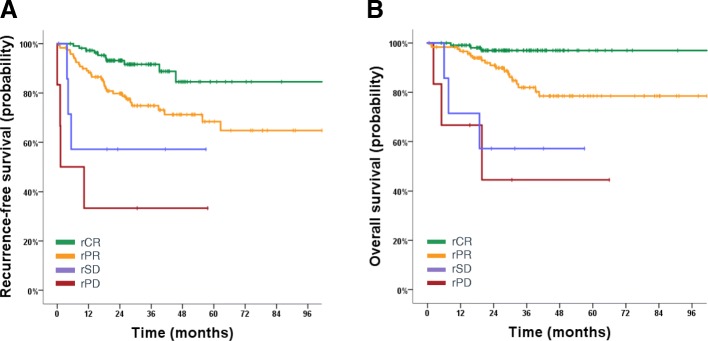
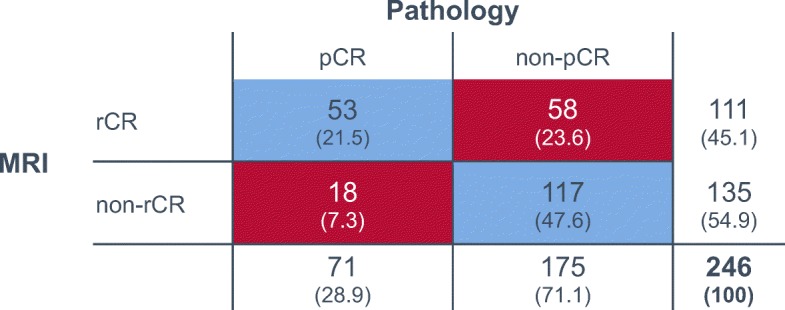
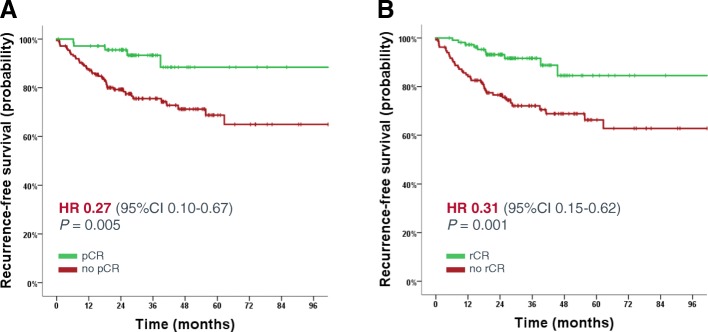
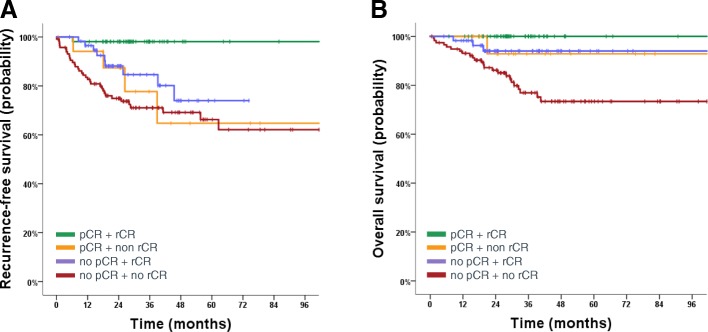
Overall rCR and pCR (no invasive tumor in the breast and axilla (ypT0/is N0)) rates were 45% (111/246) and 29% (71/246), respectively. Only 48% (53/111; 95% CI 38-57%) of rCR corresponded to a pCR (= positive predictive value - PPV). Conversely, in 87% (117/135; 95% CI 79-92%) of patients, residual tumor observed on MRI was pathologically confirmed (= negative predictive value - NPV). Sensitivity to detect a pCR was 75% (53/71; 95% CI 63-84%), while specificity to detect residual tumor and accuracy were 67% (117/175; 95% CI 59-74%) and 69% (170/246; 95% CI 63-75%), respectively. The PPV was significantly lower in hormone-receptor (HR)-positive compared to HR-negative tumors (17/52 = 33% vs. 36/59 = 61%; P = 0.004). The concordance between rCR and pCR was low (Cohen's kappa - 0.1), however in multivariate analysis both assessments were significantly associated with RFS (rCR P = 0.037; pCR P = 0.033) and OS (rCR P = 0.033; pCR P = 0.043).
Preoperative CE-MRI did not accurately predict pCR after NACT for EBC, especially not in HR-positive tumors. However, rCR was strongly associated with favorable RFS and OS.
接受新辅助化疗(NACT)后达到病理完全缓解(pCR)的早期乳腺癌(EBC)患者预后良好。对于可以高度自信地排除残留肿瘤存在的患者,可能可以避免进行乳房手术。在这里,我们研究了对比增强磁共振成像(CE-MRI)在预测 NACT 后 pCR 和长期结局方面的诊断准确性。
对接受 NACT 后进行 CE-MRI 的 EBC 患者(包括局部晚期疾病患者)进行回顾性分析(n=246)。三位放射科医生对所有 MRI 扫描进行了盲法评估,以评估是否存在(影像学完全缓解;rCR)或不存在(非 rCR)残留对比增强。使用 Cohen 的kappa 统计量对临床和病理反应进行分类比较。使用 Kaplan-Meier 方法估计无复发生存率(RFS)和总生存率(OS)。
总体 rCR 和 pCR(乳房和腋窝无浸润性肿瘤(ypT0/isN0))率分别为 45%(246 例中有 111 例)和 29%(246 例中有 71 例)。仅 48%(53/111;95%CI 38-57%)的 rCR 与 pCR 相对应(=阳性预测值-PPV)。相反,在 87%(135 例中的 117 例;95%CI 79-92%)的患者中,MRI 上观察到的残留肿瘤在病理上得到证实(=阴性预测值-NPV)。检测 pCR 的敏感性为 75%(53/71;95%CI 63-84%),而检测残留肿瘤的特异性和准确性分别为 67%(175 例中的 117 例;95%CI 59-74%)和 69%(246 例中的 170 例;95%CI 63-75%)。激素受体(HR)阳性肿瘤的 PPV 明显低于 HR 阴性肿瘤(52 例中的 17/52=33%对 59 例中的 36/59=61%;P=0.004)。rCR 与 pCR 之间的一致性较低(Cohen 的 kappa 值为-0.1),但在多变量分析中,这两种评估均与 RFS(rCR P=0.037;pCR P=0.033)和 OS(rCR P=0.033;pCR P=0.043)显著相关。
术前 CE-MRI 不能准确预测 EBC 患者接受 NACT 后的 pCR,尤其是 HR 阳性肿瘤。然而,rCR 与良好的 RFS 和 OS 密切相关。