Hammersmith Hospital, Imperial College London, Cancer Research UK, London, United Kingdom.
Hammersmith Hospital, Imperial College London, Cancer Research UK, London, United Kingdom.
J Am Coll Cardiol. 2019 Feb 5;73(4):444-453. doi: 10.1016/j.jacc.2018.10.070.
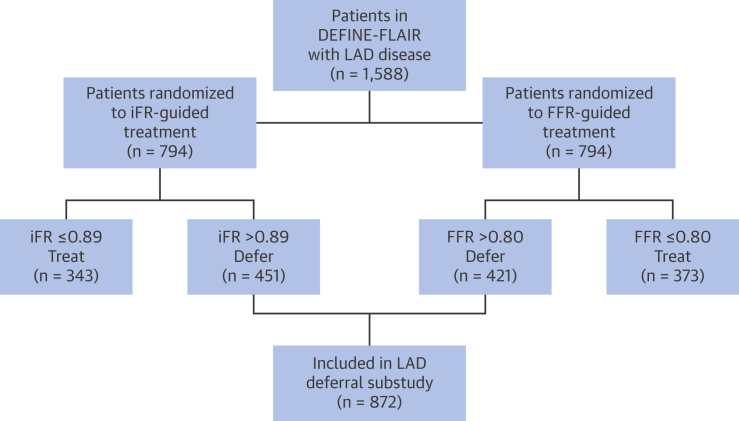
Physicians are not always comfortable deferring treatment of a stenosis in the left anterior descending (LAD) artery because of the perception that there is a high risk of major adverse cardiac events (MACE). The authors describe, using the DEFINE-FLAIR (Functional Lesion Assessment of Intermediate Stenosis to Guide Revascularisation) trial, MACE rates when LAD lesions are deferred, guided by physiological assessment using fractional flow reserve (FFR) or the instantaneous wave-free ratio (iFR).
The purpose of this study was to establish the safety of deferring treatment in the LAD using FFR or iFR within the DEFINE-FLAIR trial.
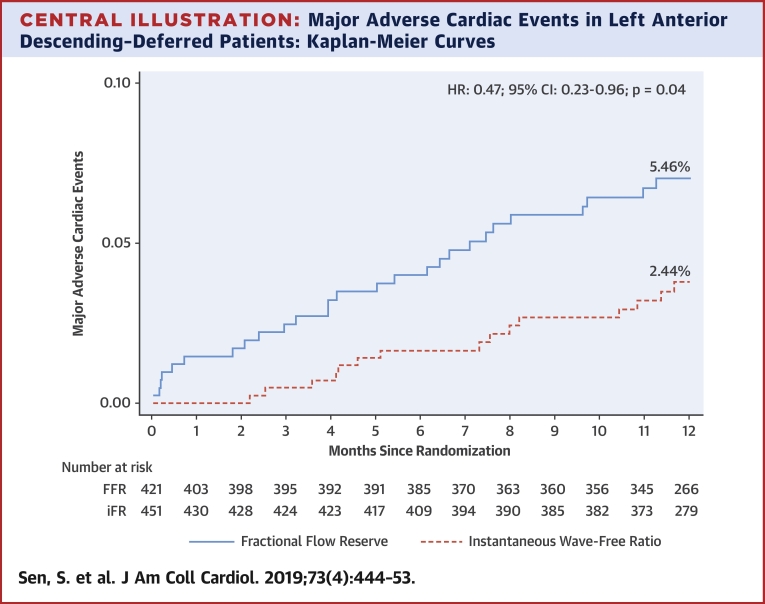
MACE rates at 1 year were compared between groups (iFR and FFR) in patients whose physiological assessment led to LAD lesions being deferred. MACE was defined as a composite of cardiovascular death, myocardial infarction (MI), and unplanned revascularization at 1 year. Patients, and staff performing follow-up, were blinded to whether the decision was made with FFR or iFR. Outcomes were adjusted for age and sex.
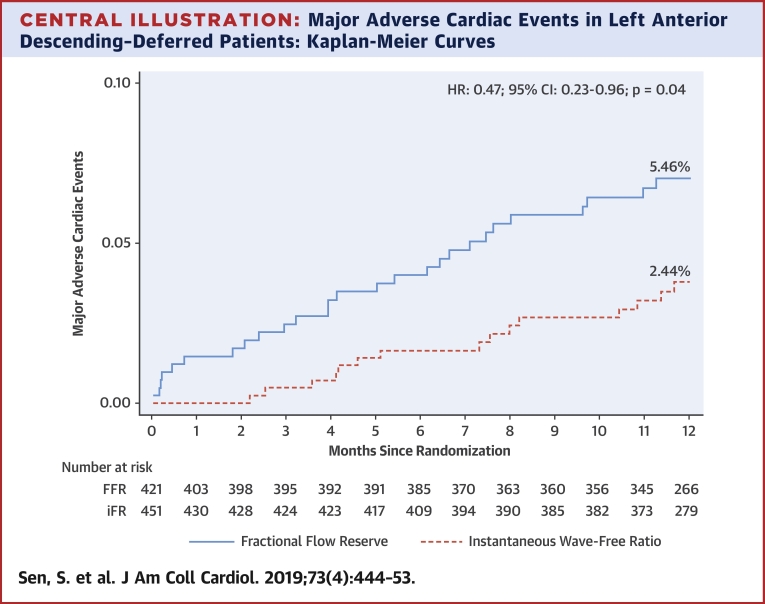
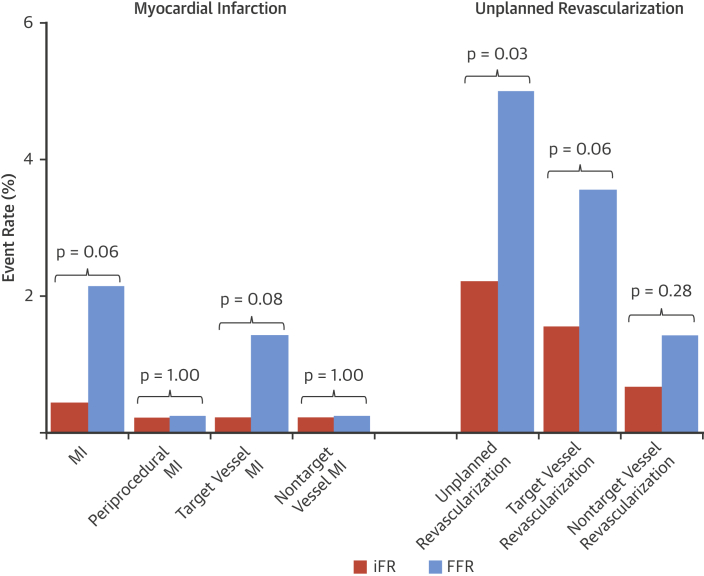
A total of 872 patients had lesions deferred in the LAD (421 guided by FFR, 451 guided by iFR). The event rate with iFR was significantly lower than with FFR (2.44% vs. 5.26%; adjusted HR: 0.46; 95% confidence interval [CI]: 0.22 to 0.95; p = 0.04). This was driven by significantly lower unplanned revascularization with iFR and numerically lower MI (unplanned revascularization: 2.22% iFR vs. 4.99% FFR; adjusted HR: 0.44; 95% CI: 0.21 to 0.93; p = 0.03; MI: 0.44% iFR vs. 2.14% FFR; adjusted HR: 0.23; 95% CI: 0.05 to 1.07; p = 0.06).
iFR-guided deferral appears to be safe for patients with LAD lesions. Patients in whom iFR-guided deferral was performed had statistically significantly lower event rates than those with FFR-guided deferral.
由于存在发生主要不良心脏事件(MACE)的高风险,医生对左前降支(LAD)狭窄的治疗往往犹豫不决。作者使用 DEFINE-FLAIR(功能性中间狭窄病变评估以指导血运重建)试验描述了使用血流储备分数(FFR)或无波比值(iFR)进行生理学评估指导下延迟治疗时 LAD 病变的 MACE 发生率。
本研究旨在确定 DEFINE-FLAIR 试验中使用 FFR 或 iFR 延迟治疗 LAD 的安全性。
比较接受生理评估后 LAD 病变延迟治疗的患者中 iFR 和 FFR 两组的 1 年 MACE 发生率。MACE 定义为 1 年内心血管死亡、心肌梗死(MI)和计划外血运重建的复合终点。患者和进行随访的工作人员对决策是使用 FFR 还是 iFR 进行了盲法。结果根据年龄和性别进行了调整。
共有 872 例患者的 LAD 病变被延迟(421 例由 FFR 指导,451 例由 iFR 指导)。iFR 组的事件发生率明显低于 FFR 组(2.44% vs. 5.26%;调整后的 HR:0.46;95%置信区间 [CI]:0.22 至 0.95;p=0.04)。这主要是由于 iFR 组的计划外血运重建显著减少,而 MI 发生率略有下降(计划外血运重建:iFR 组 2.22% vs. FFR 组 4.99%;调整后的 HR:0.44;95%CI:0.21 至 0.93;p=0.03;MI:iFR 组 0.44% vs. FFR 组 2.14%;调整后的 HR:0.23;95%CI:0.05 至 1.07;p=0.06)。
iFR 指导的延迟对 LAD 病变患者似乎是安全的。与 FFR 指导的延迟相比,iFR 指导的延迟患者的事件发生率有统计学显著降低。