Routman David M, Garant Aurelie, Lester Scott C, Day Courtney N, Harmsen William S, Sanheuza Cristobal T, Yoon Harry H, Neben-Wittich Michelle A, Martenson James A, Haddock Michael G, Hallemeier Christopher L, Merrell Kenneth W
Department of Radiation Oncology, Mayo Clinic, Rochester, Minnesota.
Department of Biomedical Statistics and Informatics, Mayo Clinic, Rochester, Minnesota.
Adv Radiat Oncol. 2019 Jan 17;4(1):63-69. doi: 10.1016/j.adro.2018.09.004. eCollection 2019 Jan-Mar.
Grade 4 lymphopenia (G4L) during radiation therapy (RT) is associated with higher rates of distant metastasis and decreased overall survival in a number of malignancies, including esophageal cancer (EC). Through a reduction in integral radiation dose, proton RT (PRT) may reduce G4L relative to photon RT (XRT). The purpose of this study was to compare G4L in patients with EC undergoing PRT versus XRT.
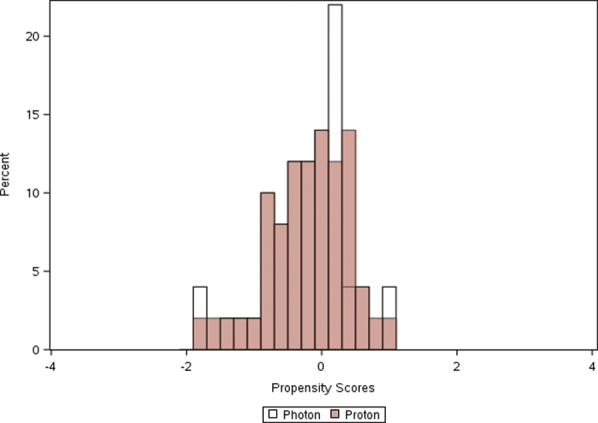
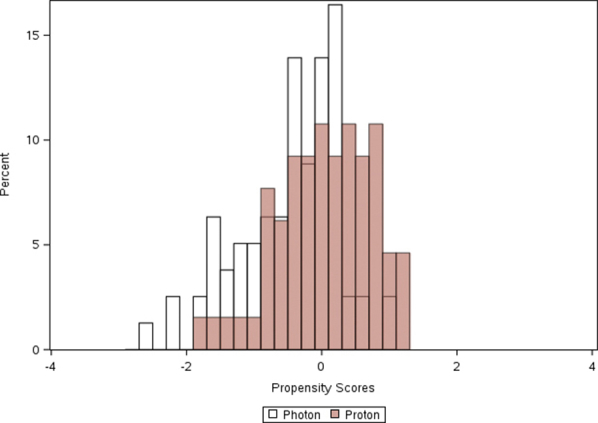
Patients receiving curative-intent RT and concurrent chemotherapy for EC were identified. Lymphocyte nadir was defined as the lowest lymphocyte count during RT. G4L was defined as absolute lymphocyte count <200/mm. Univariate and multivariable logistic regression analyses (MVA) were performed to assess patient and treatment factors associated with lymphopenia. A propensity-matched (PM) cohort was created using logistic regression, including baseline covariates.
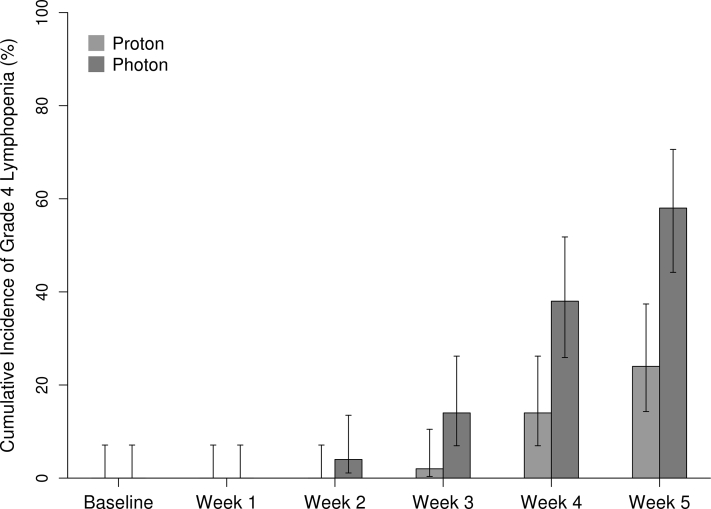
A total of 144 patients met the inclusion criteria. The median age was 66 years (range, 32-85 years). Of these patients, 79 received XRT (27% 3-dimensional chemo-RT and 73% intensity modulated RT) and 65 received PRT (100% pencil-beam scanning). Chemotherapy consisted of weekly carboplatin and paclitaxel (99%). There were no significant differences in baseline characteristics between the groups, except for age (median 4 years older in the PRT cohort). G4L was significantly higher in patients who received XRT versus those who received PRT (56% vs 22%; < .01). On MVA, XRT (odds ratio [OR]: 5.13; 95% confidence interval [CI], 2.35-11.18; < .001) and stage III/IV (OR: 4.54; 95% CI, 1.87-11.00; < .001) were associated with G4L. PM resulted in 50 PRT and 50 XRT patients. In the PM cohort, G4L occurred in 60% of patients who received XRT versus 24% of patients who received PRT. On MVA, XRT (OR: 5.28; 95% CI, 2.14-12.99; < .001) and stage III/IV (OR: 3.77; 95% CI, 1.26-11.30; = .02) were associated with G4L.
XRT was associated with a significantly higher risk of G4L in comparison with PRT. Further work is needed to evaluate a potential association between RT modality and antitumor immunity as well as long-term outcomes.
在包括食管癌(EC)在内的多种恶性肿瘤中,放射治疗(RT)期间的4级淋巴细胞减少(G4L)与远处转移率升高及总生存率降低相关。通过降低总辐射剂量,质子放疗(PRT)相对于光子放疗(XRT)可能会减少G4L。本研究的目的是比较接受PRT与XRT的EC患者的G4L情况。
确定接受EC根治性放疗及同步化疗的患者。淋巴细胞最低点定义为放疗期间的最低淋巴细胞计数。G4L定义为绝对淋巴细胞计数<200/mm³。进行单因素和多因素逻辑回归分析(MVA)以评估与淋巴细胞减少相关的患者和治疗因素。使用逻辑回归创建倾向匹配(PM)队列,包括基线协变量。
共有144例患者符合纳入标准。中位年龄为66岁(范围32 - 85岁)。这些患者中,79例接受XRT(27%为三维化疗放疗,73%为调强放疗),65例接受PRT(100%为笔形束扫描)。化疗方案为每周使用卡铂和紫杉醇(99%)。除年龄外(PRT队列中位年龄大4岁),两组间基线特征无显著差异。接受XRT患者的G4L显著高于接受PRT的患者(56%对22%;P <.01)。在MVA中,XRT(比值比[OR]:5.13;95%置信区间[CI],2.35 - 11.18;P <.001)和III/IV期(OR:4.54;CI,1.87 - 11.00;P <.001)与G4L相关。PM后有50例PRT患者和50例XRT患者。在PM队列中,接受XRT患者的G4L发生率为60%,而接受PRT患者为24%。在MVA中,XRT(OR:5.28;95%CI,2.14 - 12.99;P <.001)和III/IV期(OR:3.77;95%CI,1.26 - 11.30;P =.02)与G4L相关。
与PRT相比,XRT与G4L的风险显著更高相关。需要进一步研究以评估放疗方式与抗肿瘤免疫以及长期预后之间的潜在关联。