Department of Orthopaedics, Institute of Clinical Sciences, The Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden.
NU-Hospital Group, Trollhättan/Uddevalla, Sweden.
Knee Surg Sports Traumatol Arthrosc. 2019 Nov;27(11):3400-3410. doi: 10.1007/s00167-019-05366-w. Epub 2019 Feb 1.
This study aimed to determine the influence of femoral tunnel orientation on long-term clinical outcome and osteoarthritis in patients undergoing ACL reconstruction and to test the reliability of the implemented radiographic measurement methods. It was hypothesized that a more horizontal femoral tunnel would correlate with superior clinical outcome.
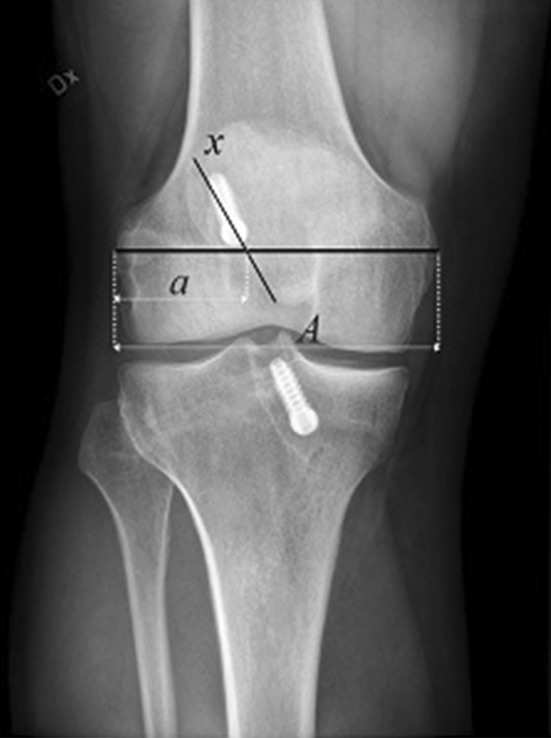
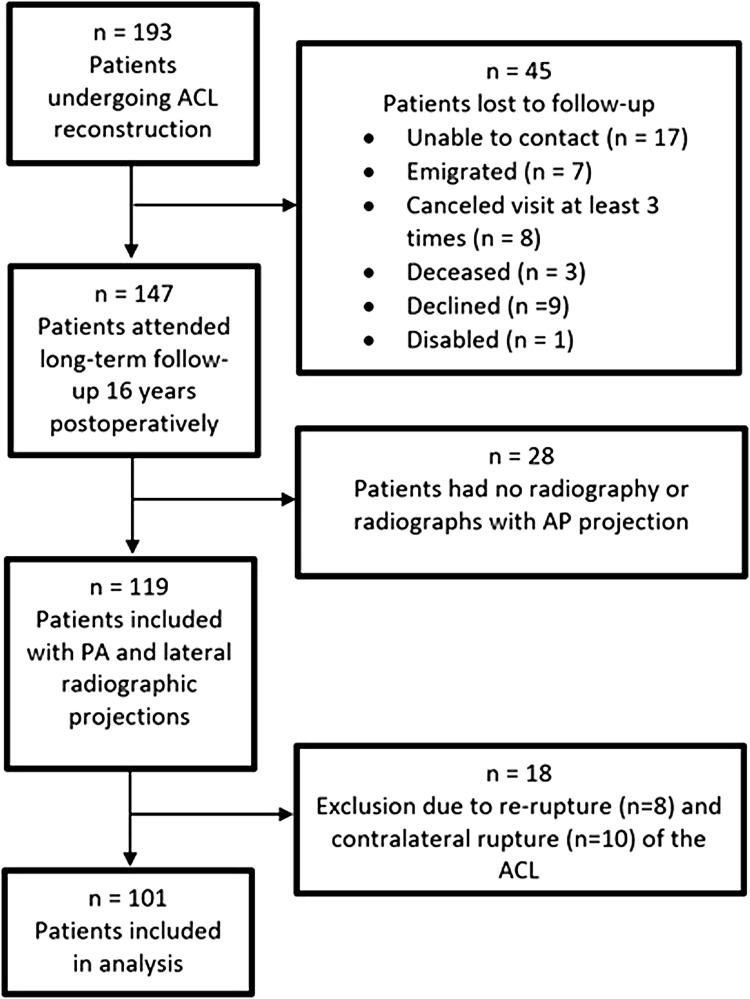
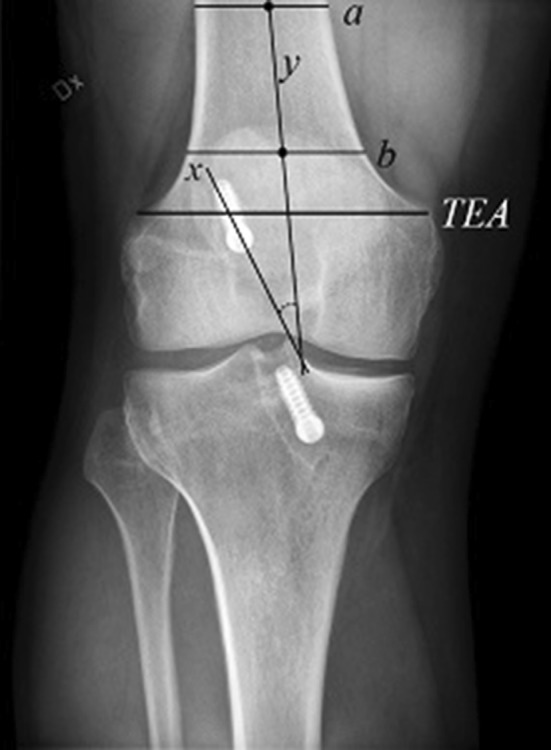
A cohort of 193 patients who underwent non-anatomic ACL reconstruction was examined. In this specific study, non-anatomic is defined by the surgeons' pursuit of optimal isometry, not to emulate the native ACL anatomy. At follow-up, the Lachman test, the KT-1000, the pivot-shift test, the one-leg-hop test and the IKDC-2000 were evaluated. Osteoarthritis was evaluated radiographically. Posteroanterior and lateral radiographs were used to determine the position of the femoral tunnel in the coronal and sagittal planes and the angle of the tunnel in the coronal plane. A method for determining femoral rotation on the lateral radiographs was developed and its reliability was evaluated. The femoral tunnel orientation was analyzed to examine its influence on clinical outcome and osteoarthritis.
A total of 101 patients were analyzed at a mean of 16.4 (± 1.3) years postoperatively. The reliability of the measurement methods was regarded as good to excellent (ICC 0.57-0.97). The mean coronal femoral tunnel angle was 9.6° (± 9.4°). The coronal femoral tunnel was positioned at a mean of 43% (± 3.5%) of the distance measured from lateral to medial. The mean sagittal femoral tunnel position, measured using the quadrant method, was 40% (± 6.4%) from posterior to anterior. No significant associations were found between tunnel orientation and the clinical outcome variables.
The orientation of the femoral tunnel did not predict the long-term subjective outcome, functional outcome or the development of osteoarthritis in patients undergoing non-anatomic ACL reconstruction. The method for determining femoral rotation on lateral radiographs was found to be reliable.
Retrospective cohort study, level of evidence IV.
本研究旨在探讨在接受 ACL 重建的患者中,股骨隧道方向对长期临床结果和骨关节炎的影响,并检验所采用的影像学测量方法的可靠性。我们假设更水平的股骨隧道会与更好的临床结果相关。
对 193 例接受非解剖 ACL 重建的患者进行了研究。在本研究中,非解剖是指外科医生追求最佳等距,而不是模拟 ACL 的解剖结构。在随访时,评估了 Lachman 试验、KT-1000、髌股关节不稳定试验、单腿跳跃试验和 IKDC-2000。通过影像学评估骨关节炎。前后位和侧位 X 线片用于确定股骨隧道在冠状面和矢状面的位置以及在冠状面的隧道角度。开发了一种用于确定侧位 X 线片上股骨旋转的方法,并对其可靠性进行了评估。分析股骨隧道方向,以检查其对临床结果和骨关节炎的影响。
共对 101 例患者进行了分析,平均随访时间为 16.4(±1.3)年。所采用的测量方法的可靠性被认为是良好到极好(ICC 0.57-0.97)。平均冠状面股骨隧道角度为 9.6°(±9.4°)。冠状面股骨隧道的位置平均为从外侧到内侧距离的 43%(±3.5%)。使用象限法测量的矢状面股骨隧道位置平均为从后向前的 40%(±6.4%)。未发现隧道方向与临床结果变量之间存在显著相关性。
在接受非解剖 ACL 重建的患者中,股骨隧道的方向并不能预测长期的主观结果、功能结果或骨关节炎的发展。在侧位 X 线片上确定股骨旋转的方法被证明是可靠的。
回顾性队列研究,证据等级 IV。