Department of Orthopaedic Surgery, Erasmus MC, University Medical Center Rotterdam, Dr. Molewaterplein 40, 3015 GD, Rotterdam, The Netherlands.
Knee Surg Sports Traumatol Arthrosc. 2022 Jun;30(6):2003-2013. doi: 10.1007/s00167-022-06871-1. Epub 2022 Feb 2.
To investigate the effect that femoral and tibial tunnel positions have on long-term reported and clinical outcome and to identify a safe zone based on favourable outcome.
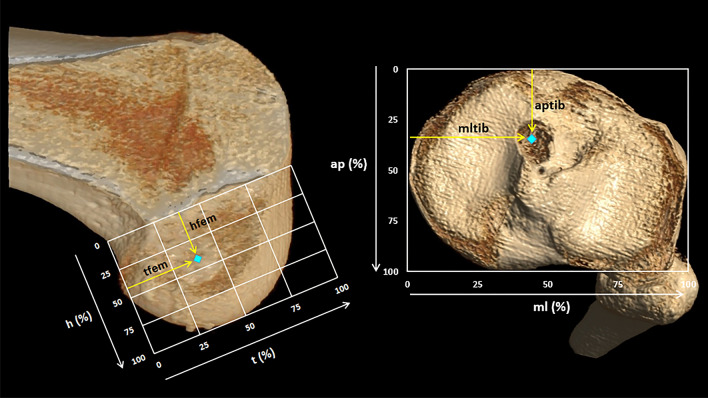
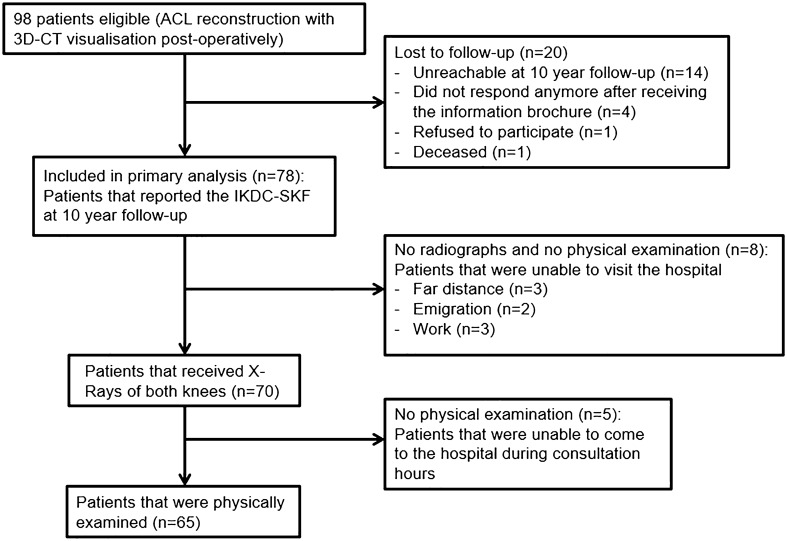
Seventy-eight patients from a previous randomised controlled trial were included and were followed with a mean follow-up of 11.4 years. All patients had primary trans-tibial anterior cruciate ligament reconstruction performed. The femoral and tibial tunnel positions were visualised and translated in percentages with three-dimensional computed tomography post-operatively. There were 3 separate outcome variables: patient-reported outcome measured with the IKDC Subjective Knee Form, overall failure, and radiographic osteoarthritis. The correlation between tunnel aperture positions and outcome was determined with multivariate regression. The area with best outcome was defined as the safe zone and was determined with Youden's index in conjunction with receiver operating characteristics.
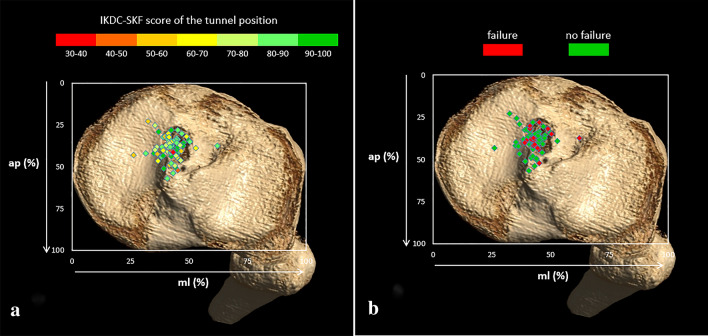
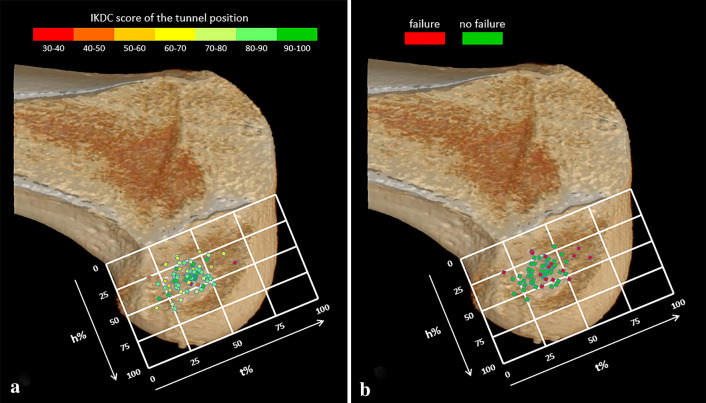
No significant relationship was found between tunnel aperture positions and IKDC Subjective Knee Form at 10-year follow-up. The posterior-to-anterior femoral tunnel aperture position parallel to Blumensaat line showed a significant relationship (p = 0.03) to overall failure at 10-year follow-up. The mean posterior-to-anterior tunnel position of the group that did not fail was 37.7% compared to 44.1% in the overall failure group. Femoral tunnel apertures placed further anteriorly had more overall failures at long-term. The cut-off point lies at 35.0% from posterior-to-anterior parallel to Blumensaat. Of the 16 overall failures, 15 (93.8%) were placed further anteriorly than the cut-off point. No significant relationship was found between tunnel aperture positions and radiographic osteoarthritis.
Femoral and tibial tunnel positions were not associated with long-term patient-reported outcome and radiographic osteoarthritis. Long-term overall failure was more frequently seen in patients with a more anteriorly placed femoral tunnel. This study identified a safe zone located at the most posterior 35% of the femoral condyle parallel to Blumensaat. This knowledge offers guidance to surgeons to operate more precisely and accurately and reconstruct a long-lasting graft.
Level III.
研究股骨和胫骨隧道位置对长期报告的临床结果的影响,并根据良好的结果确定一个安全区域。
本研究纳入了来自之前一项随机对照试验的 78 名患者,平均随访 11.4 年。所有患者均接受了经胫骨前交叉韧带重建术。术后通过三维 CT 观察并以百分比形式对股骨和胫骨隧道位置进行了测量。有 3 个独立的结果变量:使用 IKDC 主观膝关节评分测量的患者报告结果、整体失败和放射学骨关节炎。用多元回归确定隧道开口位置与结果之间的相关性。使用 Youden 指数和接收者操作特征曲线确定最佳结果的区域,定义为安全区。
在 10 年随访时,隧道开口位置与 IKDC 主观膝关节评分之间没有发现显著关系。与 Blumensaat 线平行的股骨隧道前-后开口位置与 10 年随访时的整体失败有显著关系(p=0.03)。未失败组的平均前-后隧道位置为 37.7%,而整体失败组为 44.1%。股骨隧道开口位置越靠前,长期失败的可能性越大。截断点位于距前-后平行 Blumensaat 35.0%处。在 16 例整体失败中,有 15 例(93.8%)的位置比截断点更靠前。隧道开口位置与放射学骨关节炎之间没有显著关系。
股骨和胫骨隧道位置与长期患者报告结果和放射学骨关节炎无关。股骨隧道位置越靠前,患者长期整体失败的可能性越大。本研究确定了一个安全区域,位于股骨髁最靠后的 35%处,平行于 Blumensaat。这一知识为外科医生提供了更精确和准确的操作指导,以重建持久的移植物。
III 级。