Taber David J, Gebregziabher Mulugeta, Posadas Aurora, Schaffner Caitlin, Egede Leonard E, Baliga Prabhakar K
Division of Transplant Surgery, College of Medicine, Medical University of South Carolina, Charleston, SC.
Department of Pharmacy Services, Ralph H Johnson VAMC, Charleston, SC.
J Am Coll Clin Pharm. 2018 Dec;1(2):81-88. doi: 10.1002/jac5.1024. Epub 2018 Jun 21.
Health disparities in African-American (AA) kidney transplant recipients compared with non-AA recipients are well established. Cardiovascular disease (CVD) risk control is a significant mediator of this disparity.
To assess the efficacy of improved medication safety, CVD risk control, and racial disparities in kidney transplant recipients.
Prospective, pharmacist-led, technology-aided, 6-month interventional clinical trial. A total of 60 kidney recipients with diabetes and hypertension were enrolled. Patients had to be at least one-year post transplant with stable graft function. Primary outcome measured included hypertension, diabetes, and lipid control using intent-to-treat analyses, with differences assessed between AA and non-AA recipients.
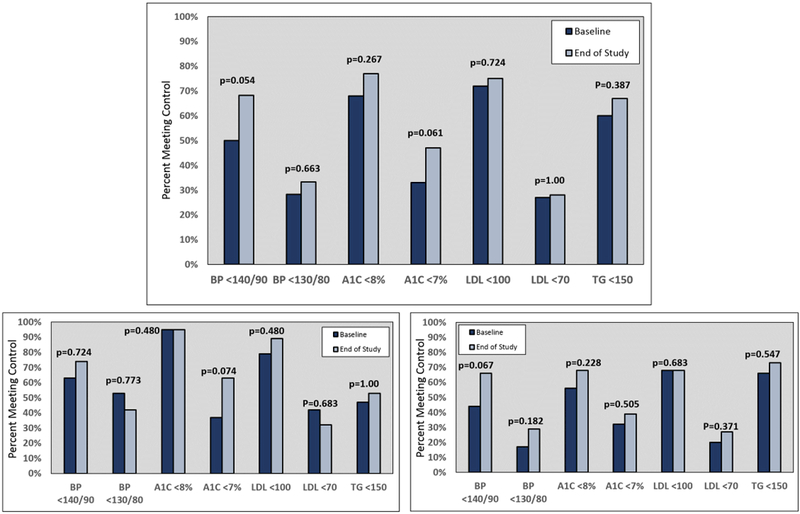
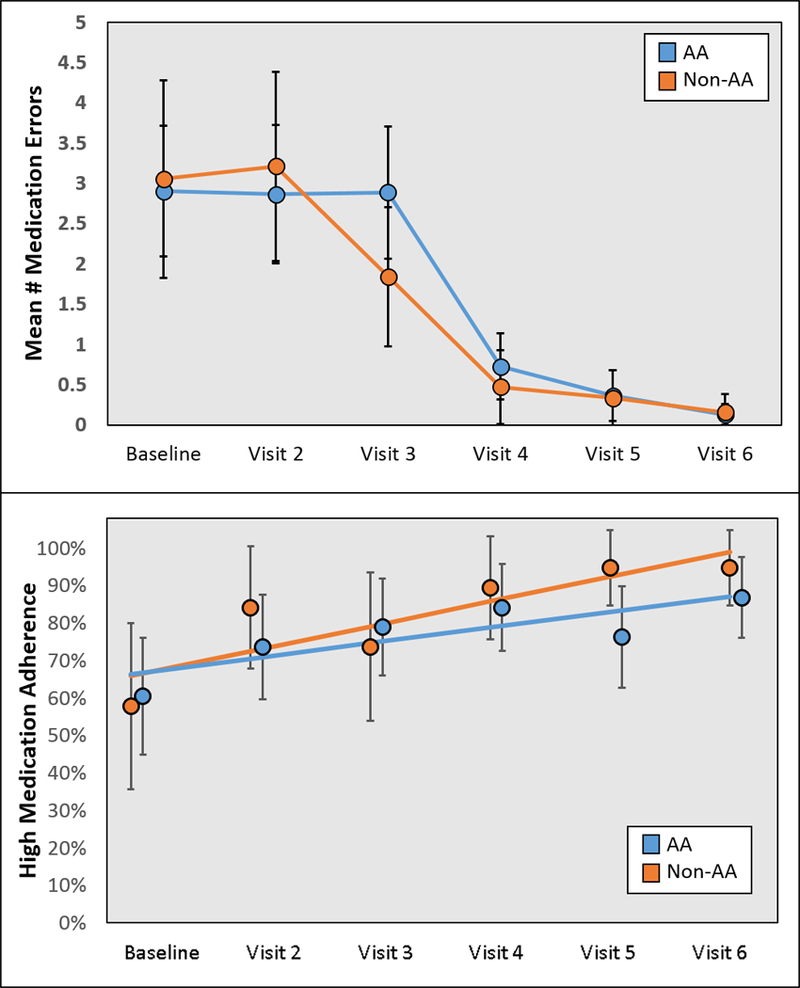
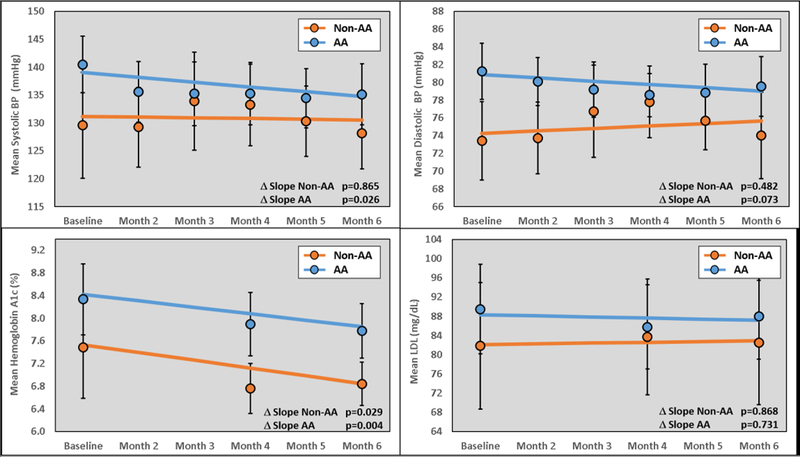
The participants mean age was 59 years, with 42% being female and 68% being AA. Overall, patients demonstrated improvements in blood pressure <140/90 mmHg (baseline 50% vs. end of study 68%, p=0.054) and hemoglobin A1c <7% (baseline 33% vs. end of study 47%, p=0.061). AAs demonstrated a significant reduction from baseline in systolic blood pressure (-0.86 mmHg per month, p=0.026), which was not evident in non-AAs (-0.13 mmHg per month, p=0.865). Mean HgbA1c decreased from baseline in the overall group (-0.12% per month, p=0.003), which was similar within AAs (-0.11% per month, p=0.004) and non-AAs (-0.14% per month, p=0.029). There were no changes in low-density lipoproteins, triglycerides, or high-density lipoproteins over the course of the study. Medication errors were significantly reduced and self-reported medication adherence significantly improved over the course of the study.
These results demonstrate the potential efficacy of a pharmacist-led, technology-aided, educational intervention in improving medication safety, diabetes, and hypertension and reducing racial disparities in AA kidney transplant recipients. (ClinicalTrials.gov NCT02763943).
与非非裔美国人(AA)肾移植受者相比,非裔美国人肾移植受者的健康差异已得到充分证实。心血管疾病(CVD)风险控制是这种差异的一个重要调节因素。
评估改善药物安全性、CVD风险控制以及肾移植受者种族差异的疗效。
前瞻性、由药剂师主导、技术辅助的6个月干预性临床试验。共纳入60例患有糖尿病和高血压的肾移植受者。患者必须在移植后至少一年且移植肾功能稳定。主要结局指标包括采用意向性分析的高血压、糖尿病和血脂控制情况,并评估AA和非AA受者之间的差异。
参与者的平均年龄为59岁,42%为女性,68%为非裔美国人。总体而言,患者的血压<140/90 mmHg有改善(基线时为50%,研究结束时为68%,p = 0.054),糖化血红蛋白<7%也有改善(基线时为33%,研究结束时为47%,p = 0.061)。非裔美国人的收缩压较基线有显著下降(每月-0.86 mmHg,p = 0.026),而非非裔美国人则不明显(每月-0.13 mmHg,p = 0.865)。总体组的平均糖化血红蛋白较基线下降(每月-0.12%,p = 0.003),在非裔美国人和非非裔美国人中相似(非裔美国人每月-0.11%,p = 0.004;非非裔美国人每月-0.14%,p = 0.029)。在研究过程中,低密度脂蛋白、甘油三酯或高密度脂蛋白无变化。在研究过程中,用药错误显著减少,自我报告的用药依从性显著提高。
这些结果表明,由药剂师主导、技术辅助的教育干预在改善非裔美国人肾移植受者的药物安全性、糖尿病和高血压以及减少种族差异方面具有潜在疗效。(ClinicalTrials.gov NCT02763943)