University of California San Francisco, San Francisco, California.
Perelman Center for Advanced Medicine, Philadelphia, Pennsylvania; Mercy Catholic Medical Center, Drexel University College of Medicine, Philadelphia, Pennsylvania.
Am J Cardiol. 2019 Apr 15;123(8):1301-1308. doi: 10.1016/j.amjcard.2019.01.025. Epub 2019 Jan 25.
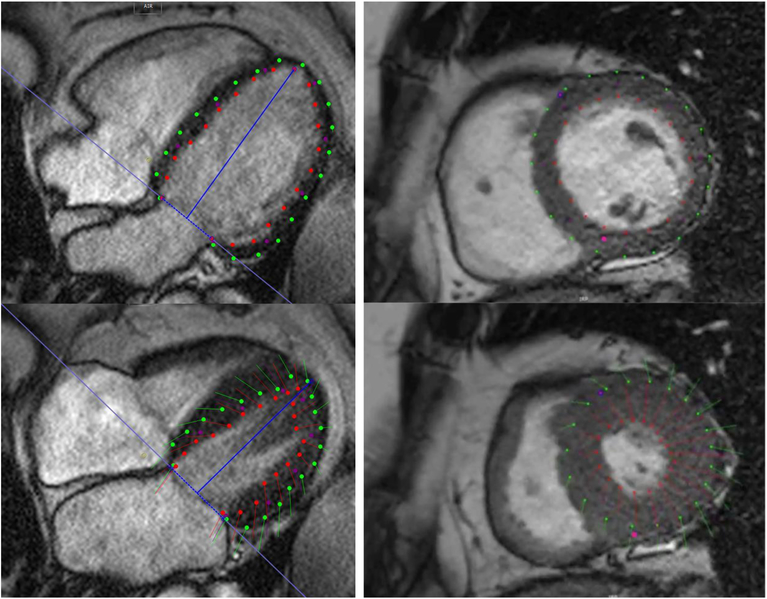
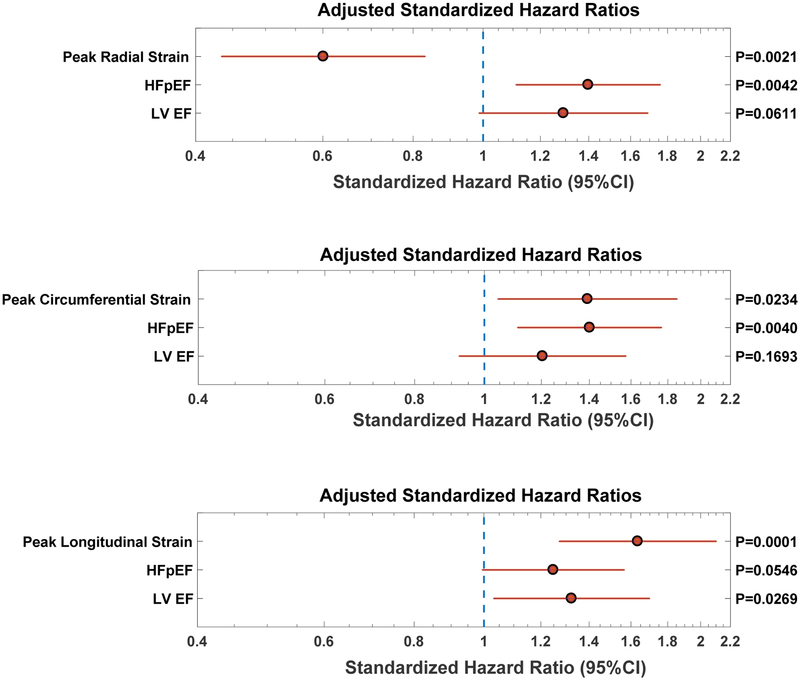
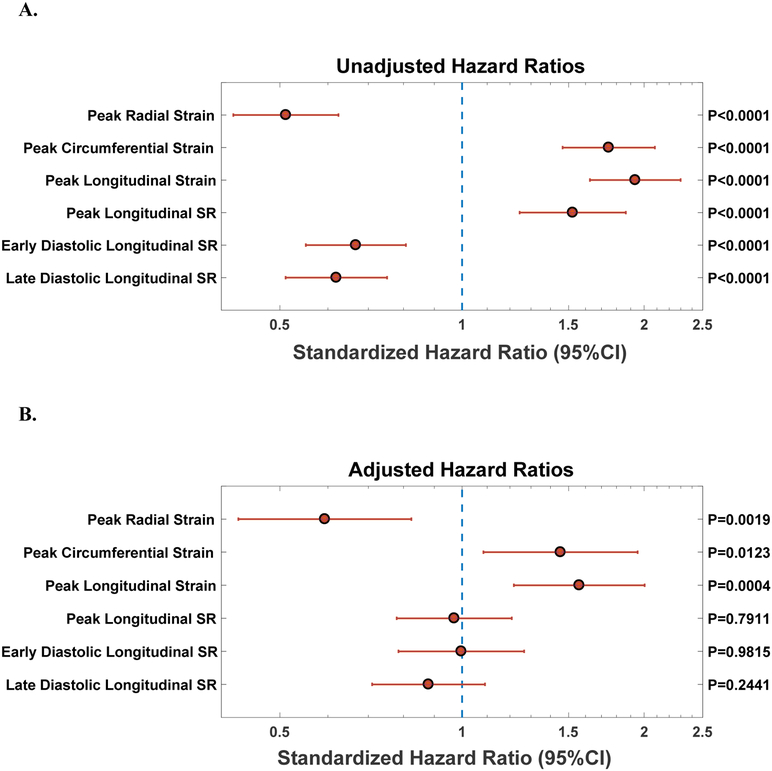
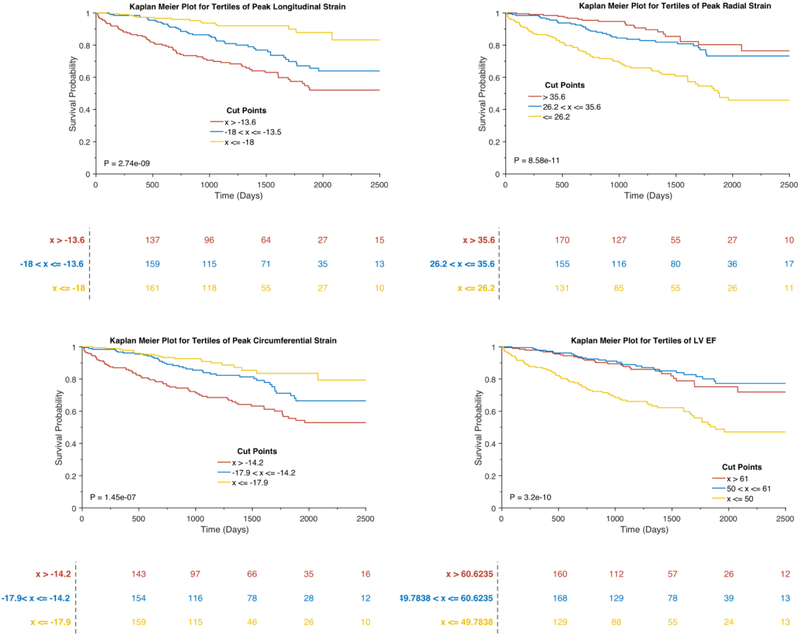
There is controversy regarding the utility of left ventricular (LV) mechanics assessed by feature-tracking steady-state free-precession (FT-SSFP), a readily implementable technique in clinical practice. In particular, whether LV mechanics assessed by FT-SSFP predicts outcomes in subjects with heart failure (HF) with reduced ejection fraction (HFrEF), with preserved ejection fraction (HFpEF), or without HF is unknown. We aimed to assess whether LV mechanics measured with FT-SSFP cine magnetic resonance imaging (MRI) predicts adverse outcomes. We prospectively enrolled 612 adults without HF (n = 402), with HF with reduced ejection fraction (HFrEF; n = 113), or HFpEF (n = 97) and assessed LV strain using FT-SSFP cine MRI. Over a median follow-up of 39.5 months, 75 participants had an HF admission, and 85 died. In Cox proportional hazards models, lower global longitudinal (Standardized hazard ratio 1.56, 95% confidence interval [CI] 1.22 to 2.00, p = 0.0004), circumferential (Standardized HR 1.46, 95% CI 1.08 to 1.95, p = 0.0123), and radial strain (Standardized HR 0.59, 95% CI 0.43 to 0.83, p = 0.0019) were independently associated with the composite endpoint, after adjustment for HF status, LV ejection fraction (LVEF), age, sex, ethnicity, body mass index, systolic and diastolic blood pressure, hypertension, diabetes, coronary artery disease, and glomerular filtration rate. Furthermore, global longitudinal strain stratified the risk of adverse outcomes across tertiles better than LVEF. In analyses that included only participants with a preserved LVEF, systolic radial, circumferential and longitudinal strain were independently predictive of adverse outcomes. We conclude that LV longitudinal, circumferential and radial strain measured using FT-SSFP cine MRI (a readily implementable technique in clinical practice) predict the risk of adverse events, independently of LVEF.
左心室(LV)力学评估采用特征追踪稳态自由进动(FT-SSFP),这是一种在临床实践中易于实施的技术,但存在争议。特别是,FT-SSFP 评估的 LV 力学是否可以预测射血分数降低的心力衰竭(HFrEF)、射血分数保留的心力衰竭(HFpEF)或无心力衰竭患者的结局尚不清楚。我们旨在评估 FT-SSFP 电影磁共振成像(MRI)测量的 LV 力学是否可以预测不良结局。我们前瞻性纳入了 612 名无心力衰竭(HF)的成年人(n=402)、射血分数降低的心力衰竭(HFrEF;n=113)或 HFpEF(n=97)患者,并使用 FT-SSFP 电影 MRI 评估 LV 应变。在中位数为 39.5 个月的随访中,75 名患者发生 HF 入院,85 名患者死亡。在 Cox 比例风险模型中,较低的整体纵向(标准化风险比 1.56,95%置信区间 [CI] 1.22 至 2.00,p=0.0004)、周向(标准化 HR 1.46,95%CI 1.08 至 1.95,p=0.0123)和径向应变(标准化 HR 0.59,95%CI 0.43 至 0.83,p=0.0019)与复合终点独立相关,调整 HF 状态、左心室射血分数(LVEF)、年龄、性别、种族、体重指数、收缩压和舒张压、高血压、糖尿病、冠状动脉疾病和肾小球滤过率后。此外,全球纵向应变比 LVEF 更能分层不良结局的风险。在仅包括保留 LVEF 的患者的分析中,收缩期径向、周向和纵向应变独立预测不良结局。我们的结论是,使用 FT-SSFP 电影 MRI 测量的 LV 纵向、周向和径向应变(一种在临床实践中易于实施的技术)可独立预测不良事件的风险,与 LVEF 无关。