Chen Siteng, Zhang Ning, Shao Jialiang, Wang Tao, Wang Xiang
Department of Urology, Shanghai General Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, China.
J Cancer. 2019 Jan 1;10(3):697-707. doi: 10.7150/jca.28494. eCollection 2019.
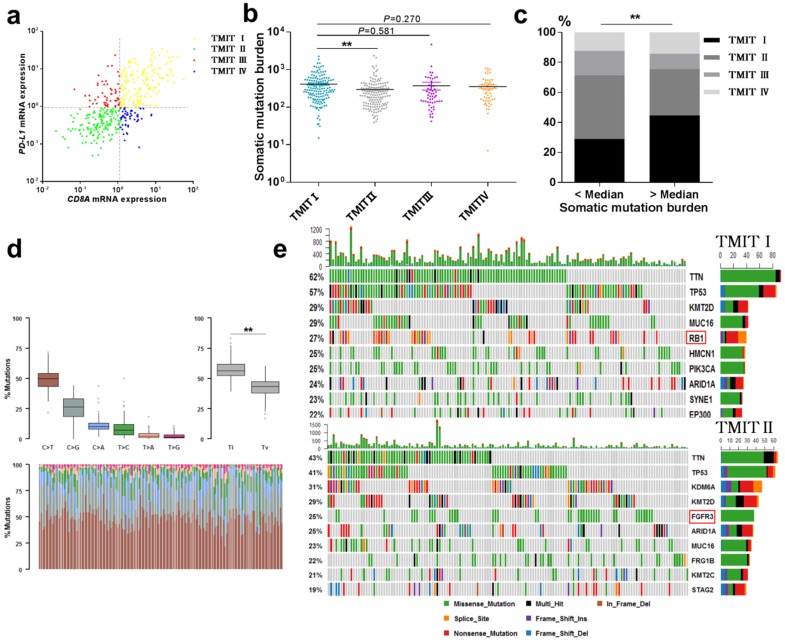
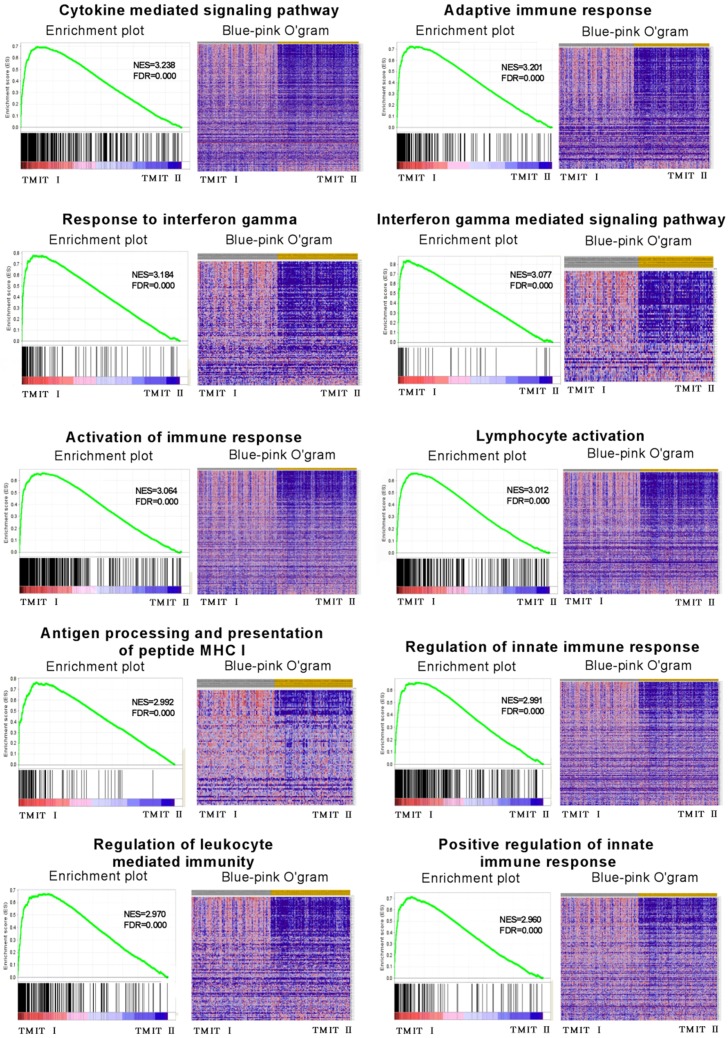
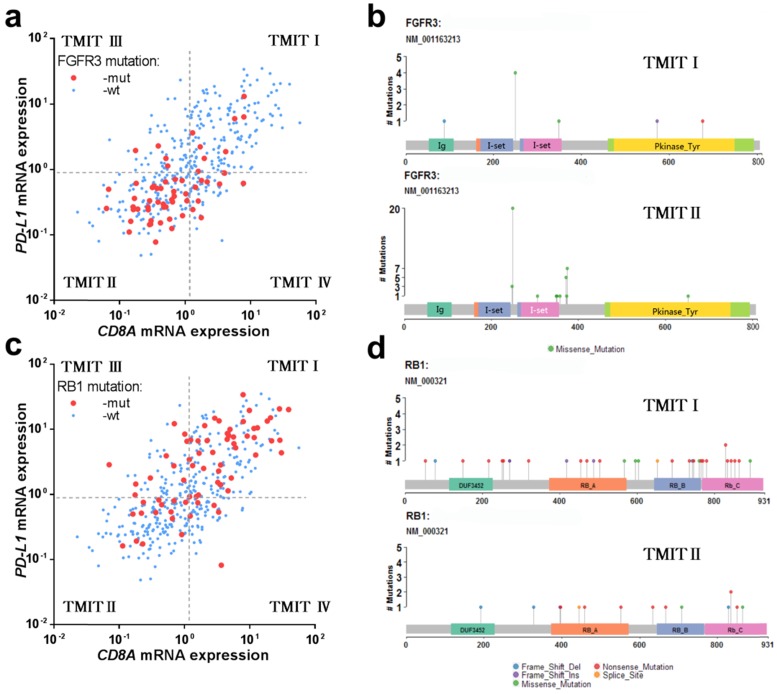
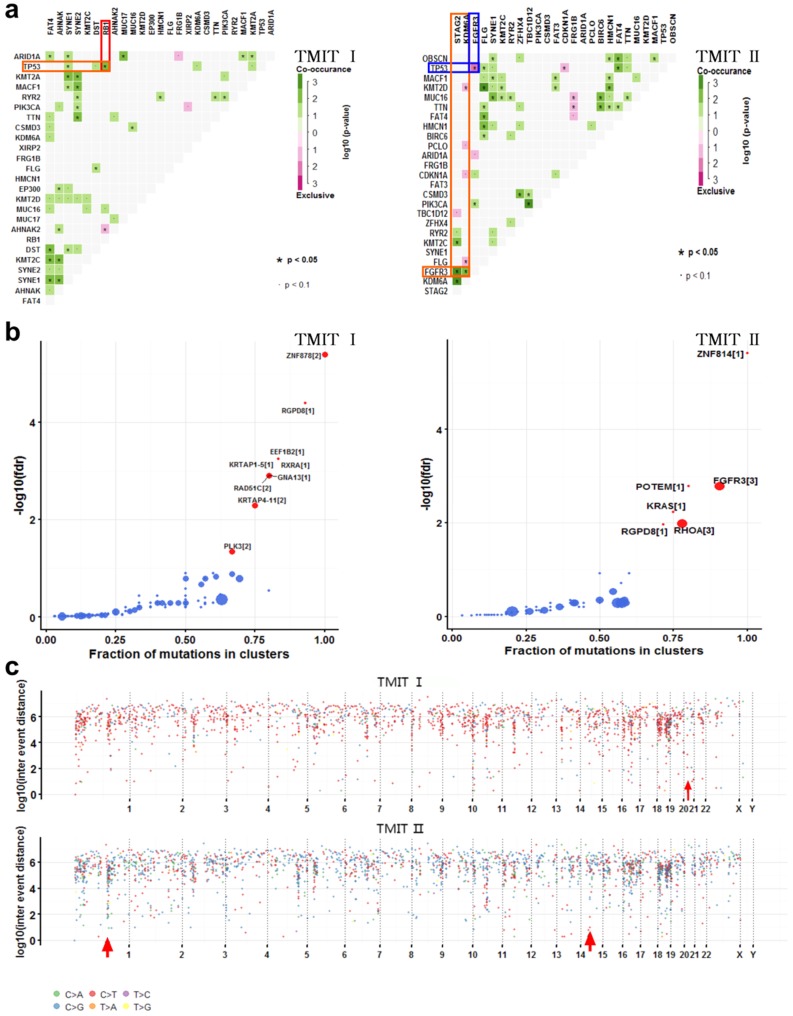
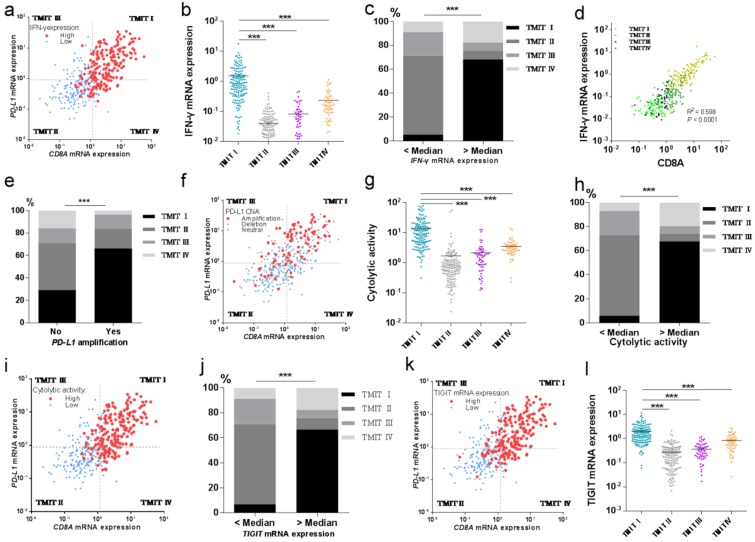
We carried out an integrated analysis based on multiple-dimensional types of data from cohorts of bladder cancer patients to identify multi-omics perspective (genomics and transcriptomics) on the tumor microenvironment on the bases of the programmed cell death 1 ligand (PD-L1) and CD8 T-cell infiltration in urothelial carcinoma. Multiple-dimensional types of data, including clinical, genomic and transcriptomic data of 408 bladder cancer patients were retrieved from the Cancer Genome Atlas database. Based on the median values of and , the tumor samples were grouped into four tumor microenvironment immune types (TMIT). The RNA sequencing profiles, somatic mutation and amplification data of bladder cancer were analyzed by different TMITs. Our research demonstrated that 36.8% of the evaluated bladder cancer belonged to TMIT I (high /high ). TIMT subtypes were not significantly associated with overall survival or disease free survival in urothelial cancer. TMIT I facilitates CD8+ T-cell infiltration and activates T-effector and interferon gamma () associated gene signature. The number of somatic mutations, cytolytic activity, mRNA expression and mRNA expression in TMIT I was remarkably higher than those in other TMIT groups. Our results showed a high rate of C>T transversion and a high rate of transition/transversion (Ti/Tv) in TMIT I bladder tumors. The mutation was significantly associated with TMIT I bladder cancer and be significantly co-occurring with the mutation. However, mutation and mutation were mutually exclusive in TMIT II bladder tumors. More importantly, different amino acid changes by mutations were also found between TMIT I and TMIT II bladder cancer, such as amino acid changes in "Immunoglobulin I-set domain (260-356)"and "Protein tyrosine kinase (472-748)". We also detected 9 genes as significantly cancer-associated genes in TMIT I bladder cancer, of which, has been reported to play an important role in DNA damage responses. Further analysis concentrated on the potential molecular mechanism found that TMIT I was significantly associated with anti-tumor immune-related signaling pathway, and was present on chromosome 21 in TMIT I bladder tumors. The classification of bladder cancer into four TMITs on the bases of the expression and the CD8+ CTLs statuses is an appropriate approach for bladder tumor immunotherapy. TMIT I (high /high ) is significantly correlated with more somatic mutation burden, and facilitates CD8+ T-cell infiltration and activates T-effector and associated gene signature. Alteration landscape for somatic variants was different between TMIT I and TMIT II (low /low ).
我们基于膀胱癌患者队列的多维数据进行了综合分析,以从程序性细胞死亡1配体(PD-L1)和尿路上皮癌中CD8 T细胞浸润的角度,确定肿瘤微环境的多组学(基因组学和转录组学)特征。从癌症基因组图谱数据库中检索了408例膀胱癌患者的多维数据,包括临床、基因组和转录组数据。根据PD-L1和CD8的中位数值,将肿瘤样本分为四种肿瘤微环境免疫类型(TMIT)。对不同TMIT类型的膀胱癌RNA测序图谱、体细胞突变和PD-L1扩增数据进行了分析。我们的研究表明,36.8%的评估膀胱癌属于TMIT I型(高PD-L1/高CD8)。TMIT亚型与尿路上皮癌的总生存期或无病生存期无显著相关性。TMIT I型促进CD8+ T细胞浸润,并激活T效应细胞和干扰素γ(IFN-γ)相关基因特征。TMIT I型中的体细胞突变数量、细胞溶解活性、PD-L1 mRNA表达和IFN-γ mRNA表达显著高于其他TMIT组。我们的结果显示,TMIT I型膀胱肿瘤中C>T颠换率和转换/颠换(Ti/Tv)率较高。TP53突变与TMIT I型膀胱癌显著相关,且与KRAS突变显著共发生。然而,TP53突变和KRAS突变在TMIT II型膀胱肿瘤中相互排斥。更重要的是,在TMIT I型和TMIT II型膀胱癌之间还发现了由TP53突变引起的不同氨基酸变化,如“免疫球蛋白I-set结构域(260-356)”和“蛋白酪氨酸激酶(472-748)”中的氨基酸变化。我们还在TMIT I型膀胱癌中检测到9个基因作为显著的癌症相关基因,其中,ATR已被报道在DNA损伤反应中起重要作用。进一步针对潜在分子机制的分析发现,TMIT I型与抗肿瘤免疫相关信号通路显著相关,且ATR存在于TMIT I型膀胱肿瘤的21号染色体上。基于PD-L1表达和CD8+ CTLs状态将膀胱癌分为四种TMIT类型是膀胱肿瘤免疫治疗的一种合适方法。TMIT I型(高PD-L1/高CD8)与更高的体细胞突变负担显著相关,促进CD8+ T细胞浸润,并激活T效应细胞和IFN-γ相关基因特征。TMIT I型和TMIT II型(低PD-L1/低CD8)之间的体细胞变异改变格局不同。