Sun Xue-Rong, Tian Ying, Shah Ashok, Yin Xian-Dong, Shi Liang, Wang Yan-Jiang, Liu Xiao-Qing, Hocini Meleze, Haissaguerre Michel, Yang Xin-Chun, Liu Xing-Peng
Heart Center, Beijing Chao-Yang Hospital, Capital Medical University, Beijing 100020, China.
Service de Rhythmologie, Hopital Cardiologique du Haut-Lévêque, Bordeaux 33000, France.
Cardiol Res Pract. 2019 Jan 2;2019:3210803. doi: 10.1155/2019/3210803. eCollection 2019.
In patients with persistent atrial fibrillation (AF), the procedural and clinical outcomes of ablation combined with infusion of antiarrhythmic drug are unknown.
To determine the impact of low-dose ibutilide after circumferential pulmonary vein isolation (CPVI) and/or left atrial (LA) substrate modification on acute procedural and clinical outcome of persistent AF.
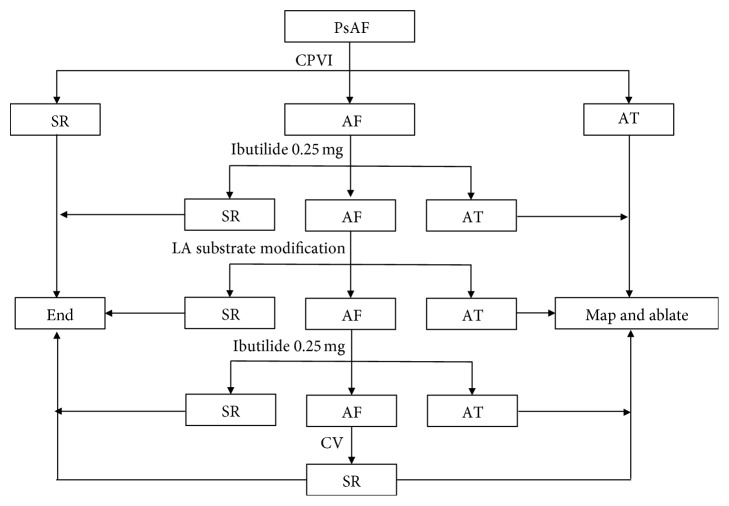
In a prospective cohort of 135 consecutive patients with persistent AF, intravenous 0.25 mg ibutilide was administered 3 days before the procedure and intraprocedurally, if required, after CPVI and/or additional LA substrate modification of sites with continuous, rapid or fractionated, and low-voltage (0.05-0.3 mv) atrial activity.
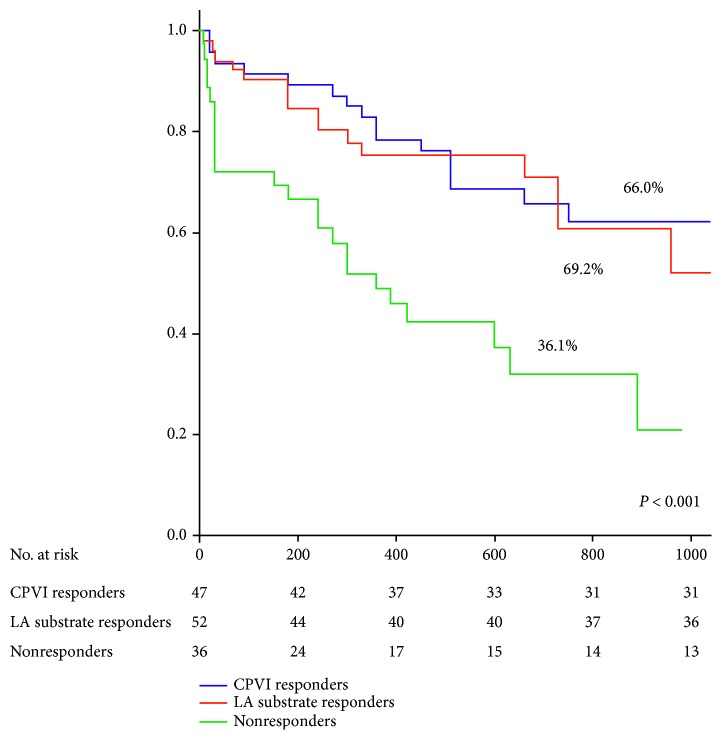
Persistent AF was terminated by CPVI alone (=15) or CPVI + ibutilide (=32) in 47 (34.8%) patients (CPVI responders). Additional LA substrate modification without (=33) or with subsequent administration of 0.25 mg ibutilide (=19) terminated AF in another 52 (38.5%) patients (substrate modification responders). Sinus rhythm was restored by electrical cardioversion in the remaining 36 (26.7%) patients (nonresponders). The mean LA substrate ablation time was 14 ± 6 minutes. At follow-up of 24 ± 10 months, the rates of freedom from atrial tachyarrhythmias among the responders in CPVI and substrate modification groups were mutually comparable (66.0% and 69.2%) and higher than among the nonresponders (36.1%; < 0.01). Among the responders, there was no difference in clinical outcome between patients whose persistent AF was terminated without or with low-dose ibutilide.
Administration of low-dose ibutilide during ablation of persistent AF may allow select patients wherein substrate ablation is not or minimally required to optimize procedural and clinical outcomes.
在持续性心房颤动(AF)患者中,消融联合输注抗心律失常药物的手术及临床效果尚不清楚。
确定在环肺静脉隔离(CPVI)和/或左心房(LA)基质改良后给予低剂量伊布利特对持续性AF急性手术及临床效果的影响。
在一个前瞻性队列中,连续纳入135例持续性AF患者,术前3天静脉给予0.25mg伊布利特,术中根据需要在CPVI和/或对具有连续、快速或碎裂及低电压(0.05 - 0.3mV)心房活动的部位进行额外LA基质改良后给予。
47例(34.8%)患者的持续性AF通过单纯CPVI(=15)或CPVI + 伊布利特(=32)终止(CPVI反应者)。另外,在未给予(=33)或随后给予0.25mg伊布利特(=19)的情况下进行LA基质改良,使另外52例(38.5%)患者的AF终止(基质改良反应者)。其余36例(26.7%)患者通过电复律恢复窦性心律(无反应者)。LA基质消融的平均时间为14±6分钟。在24±10个月的随访中,CPVI组和基质改良组反应者的房性快速心律失常无复发率相互可比(分别为66.0%和69.2%)且高于无反应者(36.1%;P<0.01)。在反应者中,持续性AF在未使用或使用低剂量伊布利特的情况下终止的患者,其临床效果无差异。
在持续性AF消融过程中给予低剂量伊布利特可能使部分患者在无需或仅需极少基质消融的情况下优化手术及临床效果。