NIHR Biomedical Research Centre and British Heart Foundation Centre of Excellence, School of Cardiovascular Medicine and Sciences, King's College London (B.N.M., H.E., R.R., D.P.).
HeartFlow Inc, Redwood City, California (S.S., H.J.K., C.R., C.A.T.).
Circ Cardiovasc Interv. 2019 Feb;12(2):e007577. doi: 10.1161/CIRCINTERVENTIONS.118.007577.
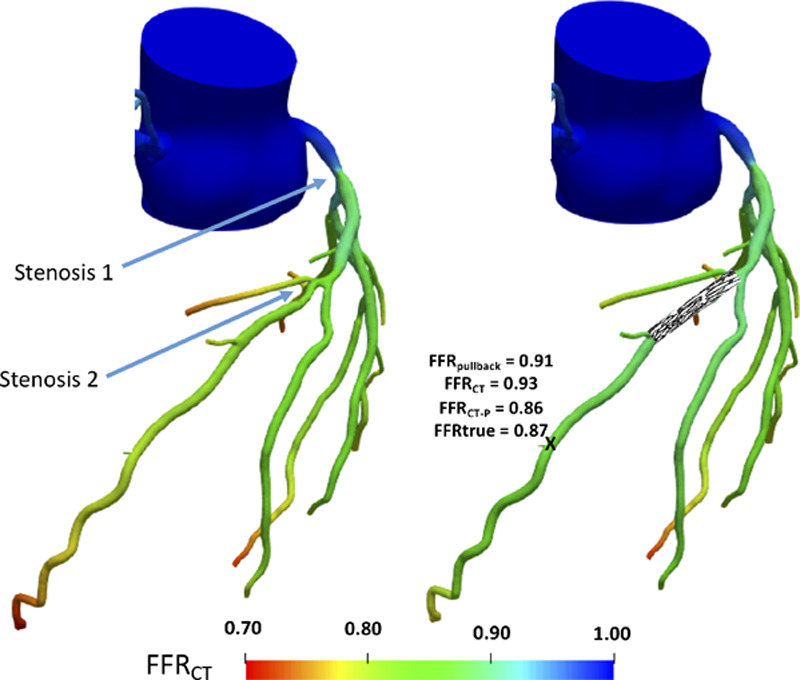
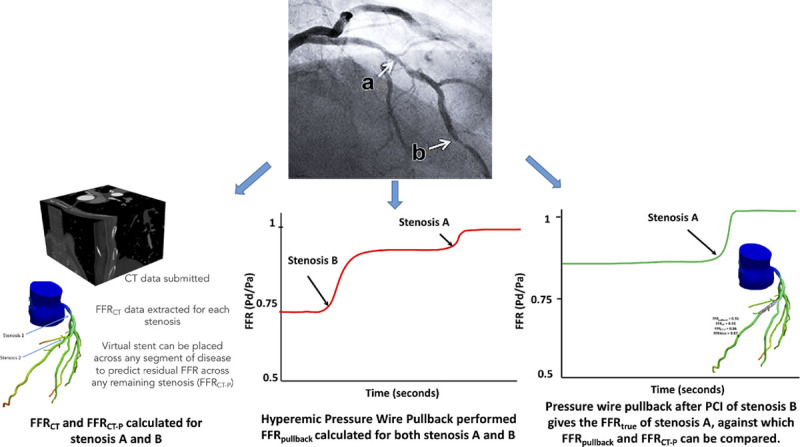
Fractional flow reserve (FFR) is commonly used to assess the functional significance of coronary artery disease but is theoretically limited in evaluating individual stenoses in serially diseased vessels. We sought to characterize the accuracy of assessing individual stenoses in serial disease using invasive FFR pullback and the noninvasive equivalent, fractional flow reserve by computed tomography (FFR). We subsequently describe and test the accuracy of a novel noninvasive FFR-derived percutaneous coronary intervention (PCI) planning tool (FFR) in predicting the true significance of individual stenoses.
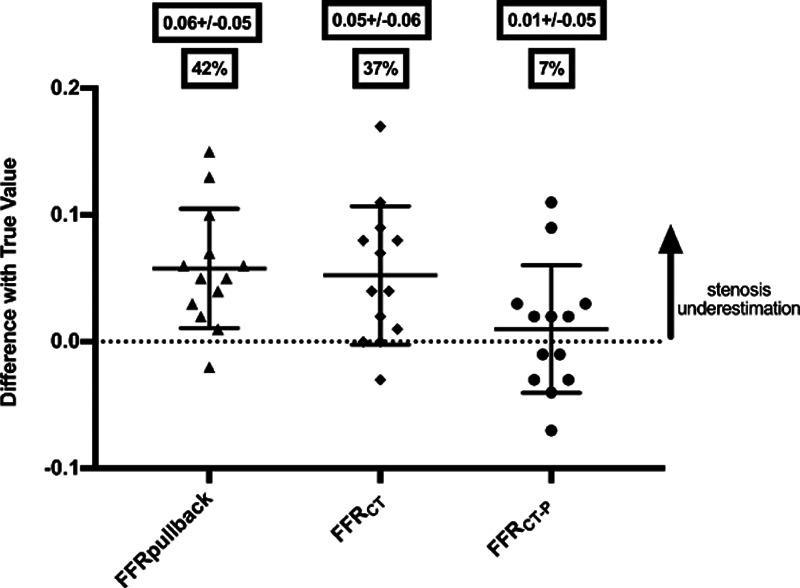
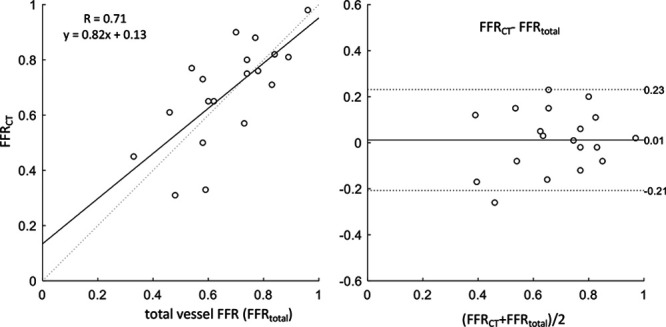
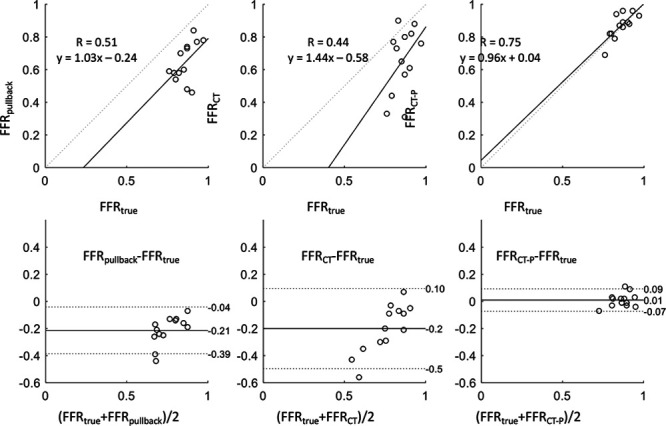
Patients with angiographic serial coronary artery disease scheduled for PCI were enrolled and underwent prospective coronary CT angiography with conventional FFR-derived post hoc for each vessel and stenosis (FFR). Before PCI, the invasive hyperemic pressure-wire pullback was performed to derive the apparent FFR contribution of each stenosis (FFR). The true FFR attributable to individual lesions (FFR) was then measured following PCI of one of the lesions. The predictive accuracy of FFR, FFR, and the novel technique (FFR) was then assessed against FFR. From the 24 patients undergoing the protocol, 19 vessels had post hoc FFR and FFR calculation. When assessing the distal effect of all lesions, FFR correlated moderately well with invasive FFR ( R=0.71; P<0.001). For lesion-specific assessment, there was significant underestimation of FFR using FFR (mean discrepancy, 0.06±0.05; P<0.001, representing a 42% error) and conventional trans-lesional FFR (0.05±0.06; P<0.001, 37% error). Using FFR, stenosis underestimation was significantly reduced to a 7% error (0.01±0.05; P<0.001).
FFR pullback and conventional FFR significantly underestimate true stenosis contribution in serial coronary artery disease. A novel noninvasive FFR-based PCI planner tool more accurately predicts the true FFR contribution of each stenosis in serial coronary artery disease.
分数血流储备(FFR)常用于评估冠状动脉疾病的功能意义,但在评估串联病变血管中的单个狭窄方面理论上存在局限性。我们试图通过有创 FFR 拖曳和无创等效物,即计算机断层扫描(CT)计算的 FFR(FFR),来描述和验证评估串联病变中单个狭窄的准确性。随后,我们描述并测试了一种新型无创 FFR 衍生的经皮冠状动脉介入治疗(PCI)规划工具(FFR)在预测单个狭窄的真实意义方面的准确性。
前瞻性纳入计划行 PCI 的串联冠状动脉疾病患者,并对每支血管和狭窄部位进行前瞻性冠状动脉 CT 血管造影和常规 FFR 后处理(FFR)。在 PCI 前,通过有创的充血压力导丝拖曳,得出每个狭窄部位的表观 FFR 贡献(FFR)。随后,在 PCI 其中一个病变后,测量个体病变的真实 FFR(FFR)。然后评估 FFR、FFR 和新型技术(FFR)的预测准确性与 FFR 的比较。从接受该方案的 24 名患者中,19 支血管有后处理 FFR 和 FFR 计算。在评估所有病变的远端影响时,FFR 与有创 FFR 相关性较好(R=0.71;P<0.001)。对于病变特异性评估,FFR 明显低估了 FFR(平均差异,0.06±0.05;P<0.001,代表 42%的误差)和传统跨病变 FFR(0.05±0.06;P<0.001,37%的误差)。使用 FFR,狭窄程度的低估明显减少到 7%的误差(0.01±0.05;P<0.001)。
FFR 拖曳和常规 FFR 明显低估了串联冠状动脉疾病中真正的狭窄程度。一种新型的无创 FFR 为基础的 PCI 规划工具更准确地预测了串联冠状动脉疾病中每个狭窄的真实 FFR 贡献。