Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, WA.
Department of Medicine, University of British Columbia, Vancouver, BC, Canada.
Blood. 2019 Apr 11;133(15):1652-1663. doi: 10.1182/blood-2018-11-883710. Epub 2019 Feb 6.
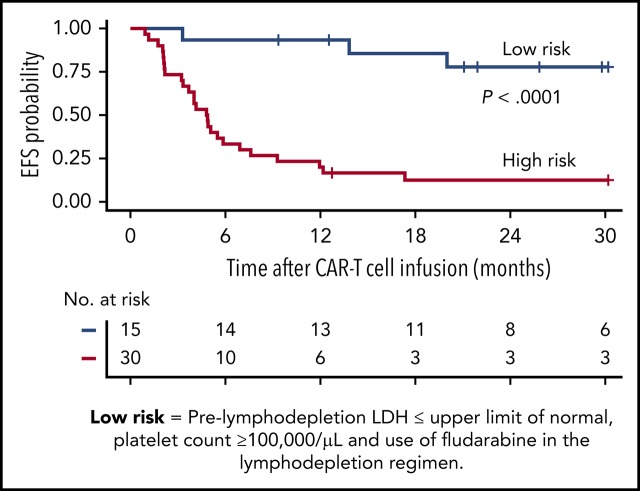
Autologous T cells engineered to express a CD19-specific chimeric antigen receptor (CAR) have produced impressive minimal residual disease-negative (MRD-negative) complete remission (CR) rates in patients with relapsed/refractory B-cell acute lymphoblastic leukemia (B-ALL). However, the factors associated with durable remissions after CAR T-cell therapy have not been fully elucidated. We studied patients with relapsed/refractory B-ALL enrolled in a phase 1/2 clinical trial evaluating lymphodepletion chemotherapy followed by CD19 CAR T-cell therapy at our institution. Forty-five (85%) of 53 patients who received CD19 CAR T-cell therapy and were evaluable for response achieved MRD-negative CR by high-resolution flow cytometry. With a median follow-up of 30.9 months, event-free survival (EFS) and overall survival (OS) were significantly better in the patients who achieved MRD-negative CR compared with those who did not (median EFS, 7.6 vs 0.8 months; < .0001; median OS, 20.0 vs 5.0 months; = .014). In patients who achieved MRD-negative CR by flow cytometry, absence of the index malignant clone by deep sequencing was associated with better EFS ( = .034). Stepwise multivariable modeling in patients achieving MRD-negative CR showed that lower prelymphodepletion lactate dehydrogenase concentration (hazard ratio [HR], 1.38 per 100 U/L increment increase), higher prelymphodepletion platelet count (HR, 0.74 per 50 000/μL increment increase), incorporation of fludarabine into the lymphodepletion regimen (HR, 0.25), and allogeneic hematopoietic cell transplantation (HCT) after CAR T-cell therapy (HR, 0.39) were associated with better EFS. These data allow identification of patients at higher risk of relapse after CAR T-cell immunotherapy who might benefit from consolidation strategies such as allogeneic HCT. This trial was registered at www.clinicaltrials.gov as #NCT01865617.
经基因工程改造表达 CD19 特异性嵌合抗原受体 (CAR) 的自体 T 细胞在复发/难治性 B 细胞急性淋巴细胞白血病 (B-ALL) 患者中产生了令人印象深刻的微小残留病灶阴性 (MRD 阴性) 完全缓解 (CR) 率。然而,CAR T 细胞治疗后持久缓解的相关因素尚未完全阐明。我们研究了在我们机构进行的评估淋巴耗竭化疗后接受 CD19 CAR T 细胞治疗的复发/难治性 B-ALL 患者,这些患者参加了一项 1/2 期临床试验。在可评估反应的 53 例接受 CD19 CAR T 细胞治疗的患者中,45 例 (85%) 通过高分辨率流式细胞术达到了 MRD 阴性 CR。中位随访 30.9 个月后,与未达到 MRD 阴性 CR 的患者相比,达到 MRD 阴性 CR 的患者无事件生存 (EFS) 和总生存 (OS) 显著改善 (中位 EFS,7.6 与 0.8 个月;<0.0001;中位 OS,20.0 与 5.0 个月;=0.014)。在通过流式细胞术达到 MRD 阴性 CR 的患者中,深度测序显示不存在指数恶性克隆与更好的 EFS 相关(=0.034)。在达到 MRD 阴性 CR 的患者中进行逐步多变量建模显示,淋巴耗竭前乳酸脱氢酶浓度较低 (危险比 [HR],每增加 100 U/L 增加 1.38)、淋巴耗竭前血小板计数较高 (HR,每增加 50000/μL 增加 0.74)、氟达拉滨纳入淋巴耗竭方案 (HR,0.25)和 CAR T 细胞治疗后异基因造血细胞移植 (HCT) (HR,0.39)与更好的 EFS 相关。这些数据允许确定 CAR T 细胞免疫治疗后复发风险较高的患者,他们可能受益于巩固策略,如异基因 HCT。该试验在 www.clinicaltrials.gov 注册,编号为 #NCT01865617。