Nuclear Medicine Department, Henri Becquerel Cancer Center, Rouen, France.
QuantIF-LITIS (EA 4108-FR CNRS 3638), Faculty of Medicine, University of Rouen, Rouen, France.
PLoS One. 2019 Feb 7;14(2):e0211649. doi: 10.1371/journal.pone.0211649. eCollection 2019.
The study objective was to compare the prognostic value of interim and end-of-treatment FDG PET/CT using five therapeutic evaluation criteria in patients with diffuse large B cell lymphoma (DLBCL).
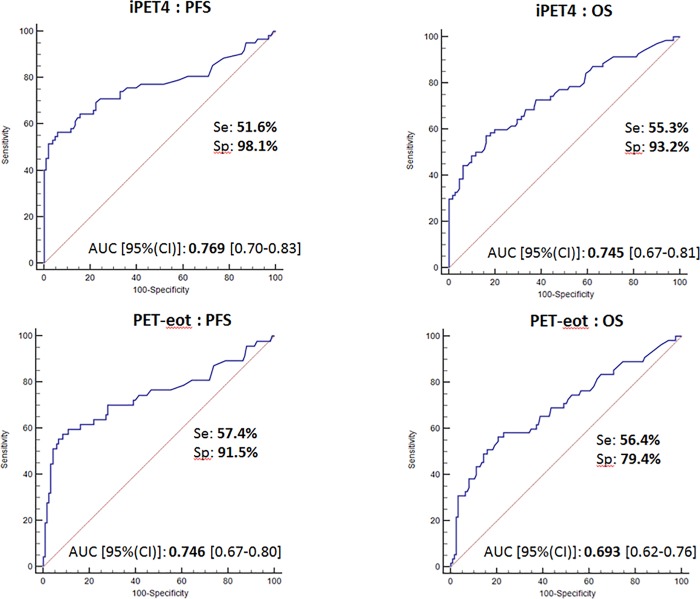
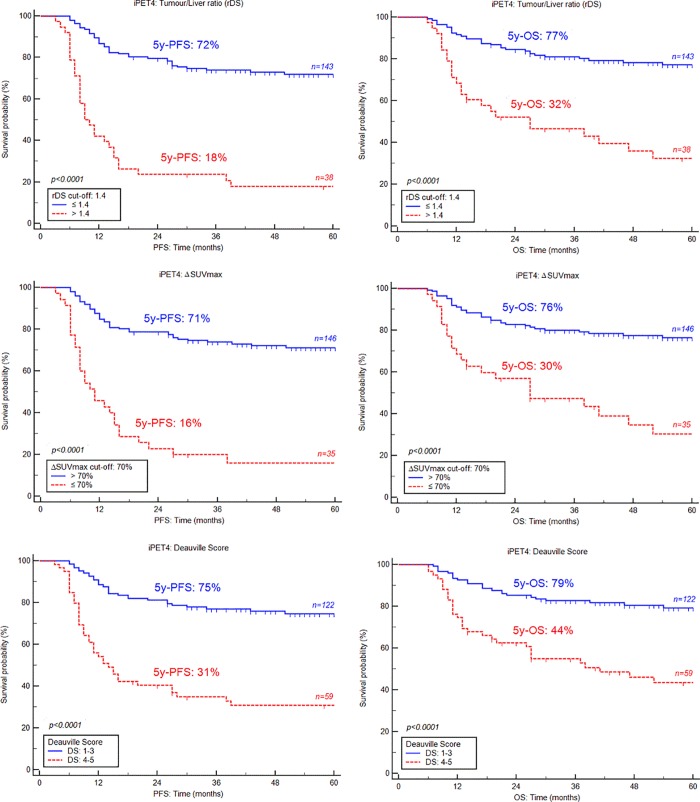
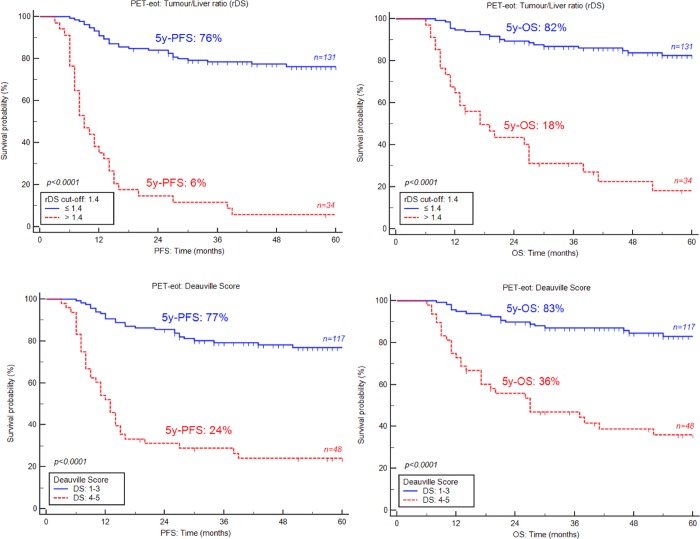
181 patients were retrospectively analysed. All patients underwent FDG-PET at baseline and after four cycles (iPET4) of first-line chemotherapy and 165 at the end-of-treatment (PET-eot). Ratio Deauville score (rDS) (SUVmax-target residual lesion/SUVmax-liver) was measured in iPET4 and PET-eot, and its optimal threshold was determined using receiver operating characteristic (ROC) curve analysis. Deauville score (DS) (iPET4 and PET-eot), ΔSUVmax, ΔSUVmax determined according to Menton 2011 criteria (ΔSUVmax+DS) and ΔSUVmax+rDS were also evaluated (iPET4 only). Median follow-up was 44 months.
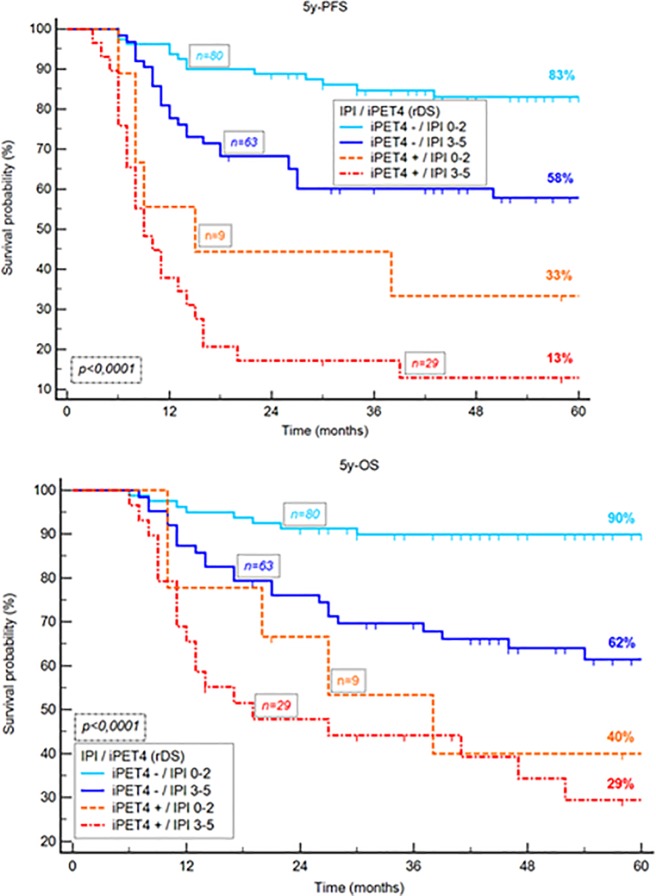
ROC analysis revealed the optimal cut-off value was 1.4-fold of SUVmax-liver on iPET4 and PET-eot. On iPET4, positive predictive value (PPV) of rDS was significantly better than DS: 81.58% vs. 67.79%. In univariate analysis, the five interpretation methods were statistically significant (p<0.0001 for progression-free survival [PFS] and overall survival [OS]). In multivariate analysis, only rDS was an independent prognostic factor (p = 0.0002 and p<0.0001 for PFS and OS, respectively). On PET-eot, similarly, the two therapeutic evaluation criteria analysed (rDS and DS) were statistically significant at the univariate level (p<0.0001). rDS was the only significant prognostic factor in multivariate analysis (p<0.0001). PPV and accuracy of rDS were also better than DS.
rDS with a tumor/liver ratio of 1.4 is a robust prognostic factor in patients with DLBCL on iPET4 and PET-eot.
本研究旨在比较使用五种治疗评估标准的中期和治疗结束时 FDG PET/CT 在弥漫性大 B 细胞淋巴瘤(DLBCL)患者中的预后价值。
回顾性分析了 181 例患者。所有患者均在基线时、一线化疗 4 个周期后(iPET4)和治疗结束时(PET-eot)进行 FDG-PET 检查。在 iPET4 和 PET-eot 中测量比值 Deauville 评分(rDS)(SUVmax-目标残留病灶/SUVmax-肝脏),并通过接受者操作特征(ROC)曲线分析确定其最佳阈值。还评估了 Deauville 评分(DS)(iPET4 和 PET-eot)、ΔSUVmax、根据 Menton 2011 标准确定的 ΔSUVmax+DS 和 ΔSUVmax+rDS(仅 iPET4)。中位随访时间为 44 个月。
ROC 分析显示,iPET4 和 PET-eot 的最佳截断值为 SUVmax-肝脏的 1.4 倍。在 iPET4 上,rDS 的阳性预测值(PPV)明显优于 DS:81.58%比 67.79%。在单因素分析中,五种解释方法具有统计学意义(无进展生存期[PFS]和总生存期[OS],p<0.0001)。多因素分析中,仅 rDS 是独立的预后因素(p=0.0002 和 p<0.0001,分别用于 PFS 和 OS)。在 PET-eot 上,同样,在单因素水平上,两种治疗评估标准(rDS 和 DS)均具有统计学意义(p<0.0001)。rDS 是多因素分析中唯一具有统计学意义的预后因素(p<0.0001)。rDS 的 PPV 和准确性也优于 DS。
在 iPET4 和 PET-eot 中,肿瘤/肝脏比值为 1.4 的 rDS 是 DLBCL 患者的可靠预后因素。