Pattison David A, MacFarlane Lisa L, Callahan Jason, Kane Emma L, Akhurst Timothy, Hicks Rodney J
Centre for Cancer Imaging, Peter MacCallum Cancer Centre, Melbourne, Australia.
Department of Nuclear Medicine & Specialised PET Services, Royal Brisbane & Women's Hospital, Butterfield Street, Brisbane, Australia.
EJNMMI Res. 2019 Feb 8;9(1):15. doi: 10.1186/s13550-019-0480-2.
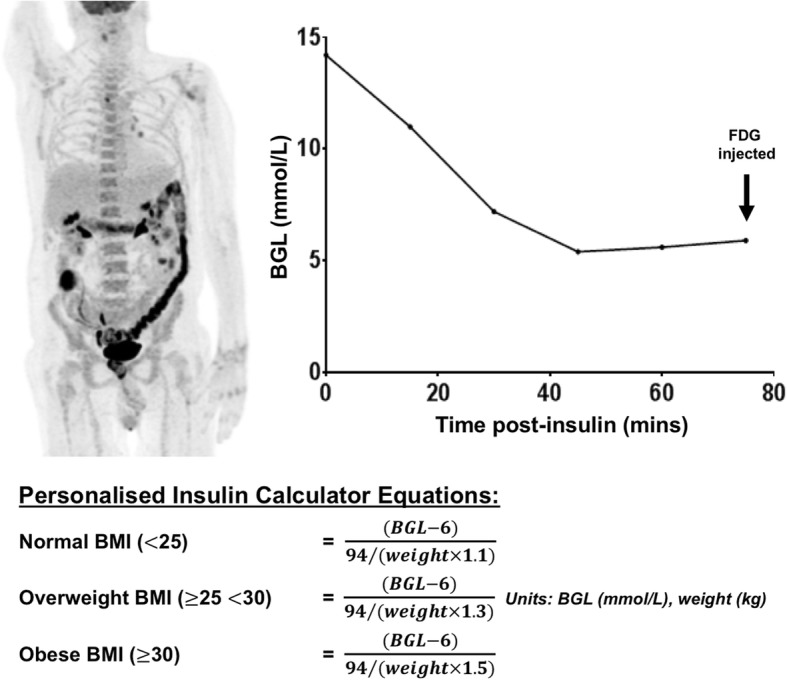
Hyperglycaemia can influence F-fluorodeoxyglucose (FDG) uptake due to competition for glucose transport and phosphorylation by hexokinase. Major international nuclear medicine societies recommend blood glucose level (BGL) < 11.1 mmol/L (200 mg/dL) prior to performing FDG positron emission tomography/computed tomography (PET/CT). However, there is no consensus approach and complications of previously proposed insulin guidelines included significant hypoglycaemia, inconvenience and skeletal muscle uptake. This study aims to establish the safety and efficacy of a personalised insulin calculator protocol to estimate the dose of intravenous insulin injection for correction of hyperglycaemia prior to FDG PET/CT.
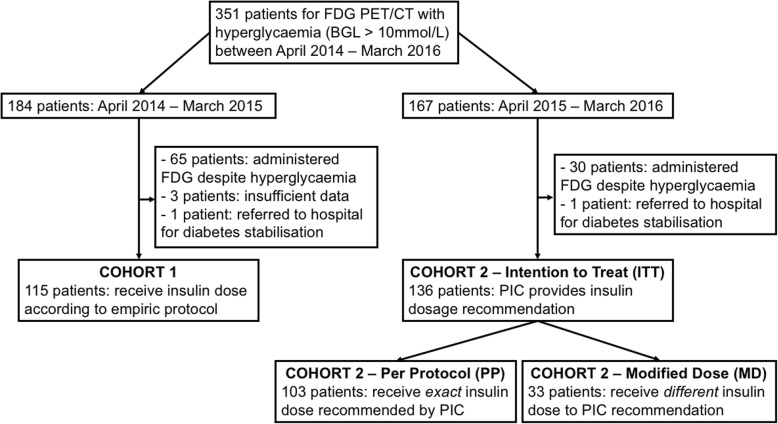
This is a retrospective audit of all patients treated with insulin for hyperglycaemia (BGL > 10 mmol/L) prior to FDG PET/CT at the Peter MacCallum Cancer Centre over a 2-year period. Cohort 1 comprised a 12-month period (April 1, 2014-March 31, 2015) using the department's established empiric-dose insulin protocol, and Cohort 2 the 12 months (April 1, 2015-March 31, 2016) following introduction of a personalised insulin calculator protocol. Variables including body mass index, insulin-dose calculated and/or administered, BGL at baseline and nadir, and time to FDG injection were analysed. There were 115 and 136 patients treated with insulin in Cohorts 1 and 2 respectively, with similar baseline variables including mean BGL (14.5 vs 14.4 mmol/L) and range (10.5-22.7 vs 10.4-24.3 mmol/L). Use of the new personalised insulin calculator resulted in significantly fewer hypoglycaemic events (0.7% vs 5.2%; P < 0.03), shorter median time from insulin to FDG injections (108 min vs 136 min; P < 0.001) and greater individualised range in insulin prescription (3-32 IU vs 4-20 IU). The majority of patients (88.3%) receiving the personalised insulin calculator prescribed dose achieved BGL < 10.0 mmol/L. All scans obtained were of diagnostic quality.
The use of our personalised insulin calculator protocol effectively lowered BGL to the target range, resulted in significantly fewer hypoglycaemic events and reduced median time between insulin and FDG injection compared to a pre-existing empiric protocol whilst achieving diagnostic scans.
高血糖可因葡萄糖转运竞争及己糖激酶磷酸化作用而影响氟脱氧葡萄糖(FDG)摄取。主要国际核医学协会建议在进行FDG正电子发射断层扫描/计算机断层扫描(PET/CT)前,血糖水平(BGL)<11.1 mmol/L(200 mg/dL)。然而,目前尚无共识性方法,且先前提出的胰岛素指南的并发症包括严重低血糖、不便及骨骼肌摄取。本研究旨在确立一种个性化胰岛素计算器方案的安全性和有效性,以估算静脉注射胰岛素剂量,用于在FDG PET/CT前纠正高血糖。
这是一项对彼得·麦卡勒姆癌症中心2年内所有在FDG PET/CT前接受胰岛素治疗高血糖(BGL>10 mmol/L)患者的回顾性审计。队列1为采用科室既定经验剂量胰岛素方案的12个月期间(2014年4月1日至2015年3月31日),队列2为引入个性化胰岛素计算器方案后的12个月(2015年4月1日至2016年3月31日)。分析了包括体重指数、计算和/或给予的胰岛素剂量、基线和最低点BGL以及FDG注射时间等变量。队列1和队列2分别有115例和136例接受胰岛素治疗的患者,基线变量相似,包括平均BGL(14.5对14.4 mmol/L)和范围(10.5 - 22.7对10.4 - 24.3 mmol/L)。使用新的个性化胰岛素计算器导致低血糖事件显著减少(0.7%对5.2%;P<0.03),从胰岛素注射到FDG注射的中位时间缩短(108分钟对136分钟;P<0.001),胰岛素处方的个体化范围更大(3 - 32 IU对4 - 20 IU)。大多数接受个性化胰岛素计算器规定剂量的患者(88.3%)BGL<10.0 mmol/L。所有获得的扫描均具有诊断质量。
与现有的经验方案相比,使用我们的个性化胰岛素计算器方案可有效将BGL降至目标范围,低血糖事件显著减少,胰岛素与FDG注射之间的中位时间缩短,同时获得诊断性扫描。