Allemann Florin, Heining Sandro, Zelle Boris, Probst Christian, Pape Hans-Christoph
1Department of Trauma, Universitaetsspital, University of Zurich, Raemistr.100, 8091 Zurich, Switzerland.
2University of Texas Science Center at San Antonio, Floyd Curl Dr., 7703, San Antonio, TX 78229 USA.
Patient Saf Surg. 2019 Feb 4;13:7. doi: 10.1186/s13037-019-0187-3. eCollection 2019.
In terms of upper extremity fractures by patients with multiple injuires, a lot of studies have assessed the functional outcome following trauma to have less favorable outcomes in regards to functional recovery. We tested the hypothesis that differences in clinical outcome occur between shaft and articular injuries of the upper extremity, when patients that sustained neurologic deficits (e.g. brachial plexus lesions) are excluded.
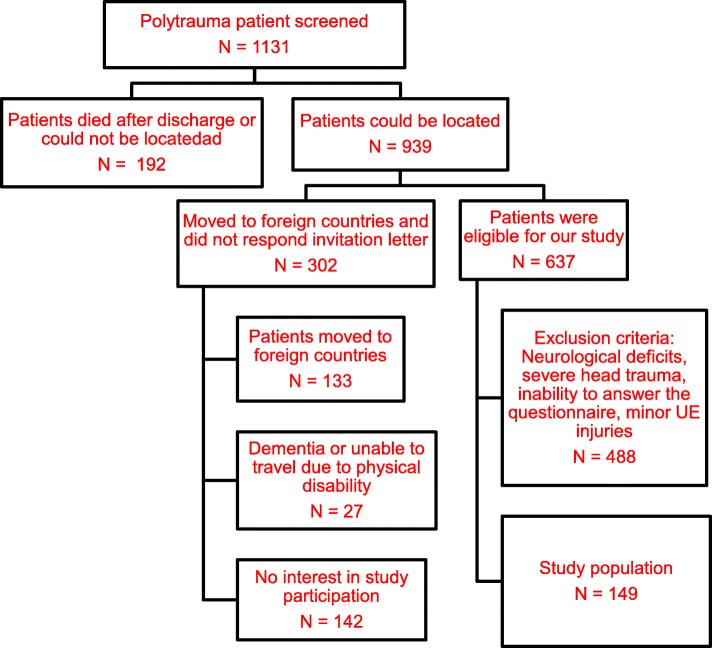
We involved Patients with isolated or combined upper extremity fracture, ISS > 16 in a level one trauma center. The follow up was at least 10 years after the initial injury. Both clinical examination (range of motion, instability, contractures, peripheral nerve damage) and radiographic analysis were carried out. We evaluated also the development of heterotopic ossifications. To analyse patients were subdivided into 3 different subgroups (articular [IA], shaft [IS], and combined [C]).
A statistically significant difference was found when ROM was compared between Group IS and C ( = 0.012), for contractures between Groups IA and C ( = 0.009) and full muscle elbow forces between Groups IS and C ( = 0.005) and Group IA and IS ( = 0.021). There was a significantly increased incidence in heterotopic ossifications when articular involvement was present. This applied for the isolated ( < 0.02) and the combined group (Group C vs Group IS, = 0.003).When Brooker type I/II in group IA and Brooker types III/IV were combined, there was a significant difference ( < 0.001). In group IA ( = 1) and in group C ( = 6), HO developed or worsened after revision surgery, all of which were performed for malunion or nonunion.
In this study, patients with isolated shaft fractures of the upper extremity tend to have a more favorable outcome in comparison with combined to isolated articular fractures in terms of range of motion, pain and the ability to use the arm for everyday activities.In the clinical practice of the treatment of polytraumatized patients with upper extremity injuries, we feel that the relevance of these injuries should not be underestimated. They are especially prone to development of heterotopic ossifications, thus requiring prophylactic measures, if necessary. As their incidence increases with the rate of reoperations, we feel that even during initial care, meticulous surgery is required to avoiding the necessity of revision surgeries. Similar to injuries below the knee, upper extremity injuries, should be treated to avoid any functional disability.
关于多发伤患者的上肢骨折,许多研究评估了创伤后的功能结局,发现功能恢复方面的结果不太理想。我们检验了这样一个假设:当排除存在神经功能缺损(如臂丛神经损伤)的患者时,上肢骨干损伤和关节损伤的临床结局存在差异。
我们纳入了一家一级创伤中心的孤立性或合并性上肢骨折、损伤严重度评分(ISS)>16的患者。随访在初次受伤后至少10年进行。进行了临床检查(活动范围、不稳定、挛缩、周围神经损伤)和影像学分析。我们还评估了异位骨化的发生情况。为了进行分析,将患者分为3个不同的亚组(关节损伤组[IA]、骨干损伤组[IS]和合并损伤组[C])。
比较IS组和C组的活动范围时发现有统计学显著差异(P=0.012),IA组和C组的挛缩情况(P=0.009)、IS组和C组以及IA组和IS组的全肌肉肘部力量(P=0.005和P=0.021)之间也有显著差异。存在关节受累时,异位骨化的发生率显著增加。这适用于孤立性关节损伤组(P<0.02)和合并损伤组(C组与IS组比较,P=0.003)。当IA组的布鲁克I/II型和III/IV型合并计算时,有显著差异(P<0.001)。在IA组(n=1)和C组(n=6)中,翻修手术后异位骨化出现或加重,所有这些翻修手术均是因为骨不连或畸形愈合而进行的。
在本研究中,与合并性或孤立性关节骨折相比,孤立性上肢骨干骨折患者在活动范围、疼痛以及使用手臂进行日常活动的能力方面往往有更有利的结局。在治疗多发伤合并上肢损伤的患者的临床实践中,我们认为这些损伤的相关性不应被低估。它们特别容易发生异位骨化,因此必要时需要采取预防措施。由于其发生率随着再次手术率的增加而上升,我们认为即使在初始治疗期间,也需要进行细致的手术以避免翻修手术的必要性。与膝部以下损伤类似,上肢损伤应得到治疗以避免任何功能残疾。