Chen Ching-Jen, Ding Dale, Ironside Natasha, Buell Thomas J, Southerland Andrew M, Woo Daniel, Worrall Bradford B
Department of Neurological Surgery, University of Virginia, Charlottesville, Virginia, USA.
Department of Neurosurgery, University of Louisville, Louisville, Kentucky, USA.
World Neurosurg. 2019 Mar;123:e700-e708. doi: 10.1016/j.wneu.2018.11.260. Epub 2019 Feb 8.
Despite no clear evidence from randomized trials, surgical intervention of spontaneous intracerebral hemorrhage (ICH) still occurs. We sought to describe the characteristics of patients undergoing surgical intervention in ICH.
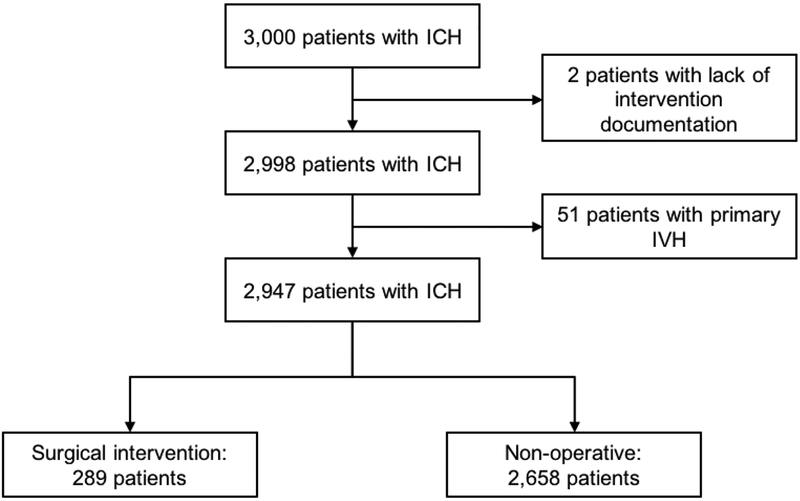
Data from the ERICH (ERICH Ethnic/Racial Variations of Intracerebral Hemorrhage) study were analyzed, and patients with ICH were categorized into surgical intervention or nonoperative management groups. Patients with primary intraventricular hemorrhage and those without data regarding the use of surgical intervention were excluded.
The study cohort comprised 2947 patients, and surgical intervention was performed in 289 (10%). Younger age (odds ratio [OR], 0.967; P < 0.001), lower baseline modified Rankin Scale score (OR, 0.728; P < 0.001), higher admission Glasgow Coma Scale score (OR, 1.059; P = 0.007), larger ICH volume (OR, 1.037; P < 0.001), infratentorial ICH location (OR, 5.966; P < 0.001), lobar ICH location (OR, 1.906; P = 0.001), lack of intraventricular hemorrhage (OR, 0.567; P = 0.001), intracranial pressure (ICP) monitoring (OR, 5.022; P < 0.001), and mannitol use (OR, 2.389; P < 0.001) were independent predictors of surgical intervention. Younger age (OR, 0.953; P < 0.001), lower baseline modified Rankin Scale score (OR, 0.713; P = 0.002), larger ICH volume (OR, 1.033; P < 0.001), lobar ICH location (OR, 2.467; P < 0.001), ICP monitoring (OR, 3.477; P < 0.001), and mannitol use (OR, 2.139; P < 0.001) were independent predictors of surgical interventions in supratentorial ICHs. Larger ICH volume (OR, 1.078; P < 0.001), ICP monitoring (OR, 6.099; P < 0.001), and mannitol use (OR, 2.952; P = 0.005) were independent predictors of surgical interventions in infratentorial ICHs.
We identified multiple factors associated with surgical intervention for patients with ICH. Younger age, good neurologic function at baseline, large ICH volume on presentation, and lobar or infratentorial hematomas were independently associated with surgical intervention in patients with ICH .
尽管随机试验尚无明确证据,但自发性脑出血(ICH)的手术干预仍在进行。我们试图描述接受ICH手术干预患者的特征。
分析来自ERICH(脑出血的种族/民族差异)研究的数据,将ICH患者分为手术干预组或非手术治疗组。排除原发性脑室出血患者及无手术干预使用数据的患者。
研究队列包括2947例患者,其中289例(10%)接受了手术干预。年龄较小(优势比[OR],0.967;P<0.001)、基线改良Rankin量表评分较低(OR,0.728;P<0.001)、入院时格拉斯哥昏迷量表评分较高(OR,1.059;P=0.007)、脑出血体积较大(OR,1.037;P<0.001)、幕下脑出血部位(OR,5.966;P<0.001)、脑叶脑出血部位(OR,1.906;P=0.001)、无脑室出血(OR,0.567;P=0.001)、颅内压(ICP)监测(OR,5.022;P<0.001)和甘露醇使用(OR,2.389;P<0.001)是手术干预的独立预测因素。年龄较小(OR,0.953;P<0.001)、基线改良Rankin量表评分较低(OR,0.713;P=0.002)、脑出血体积较大(OR,1.033;P<0.001)、脑叶脑出血部位(OR,2.467;P<0.001)、ICP监测(OR,3.477;P<0.001)和甘露醇使用(OR,2.139;P<0.001)是幕上ICH手术干预的独立预测因素。脑出血体积较大(OR,1.078;P<0.001)、ICP监测(OR,6.099;P<0.001)和甘露醇使用(OR,2.952;P=0.005)是幕下ICH手术干预的独立预测因素。
我们确定了与ICH患者手术干预相关的多个因素。年龄较小、基线神经功能良好、就诊时脑出血体积较大以及脑叶或幕下血肿与ICH患者的手术干预独立相关。