Wilkinson Thomas J, Watson Emma L, Gould Douglas W, Xenophontos Soteris, Clarke Amy L, Vogt Barbara P, Viana João L, Smith Alice C
Department of Infection, Immunity and Inflammation, University of Leicester, Leicester, UK.
Department of Clinical Medicine, Faculdade de Medicina de Botucatu, Universidade Estadual Paulista, UNESP, São Paulo, Brazil.
Clin Kidney J. 2019 Feb;12(1):113-121. doi: 10.1093/ckj/sfy071. Epub 2018 Aug 13.
Chronic kidney disease (CKD) patients experience a high symptom burden including fatigue, sleep difficulties, muscle weakness and pain. These symptoms reduce levels of physical function (PF) and activity, and contribute to poor health-related quality of life (HRQoL). Despite the gathering evidence of positive physiological changes following exercise in CKD, there is limited evidence on its effect on self-reported symptom burden, fatigue, HRQoL and physical activity.
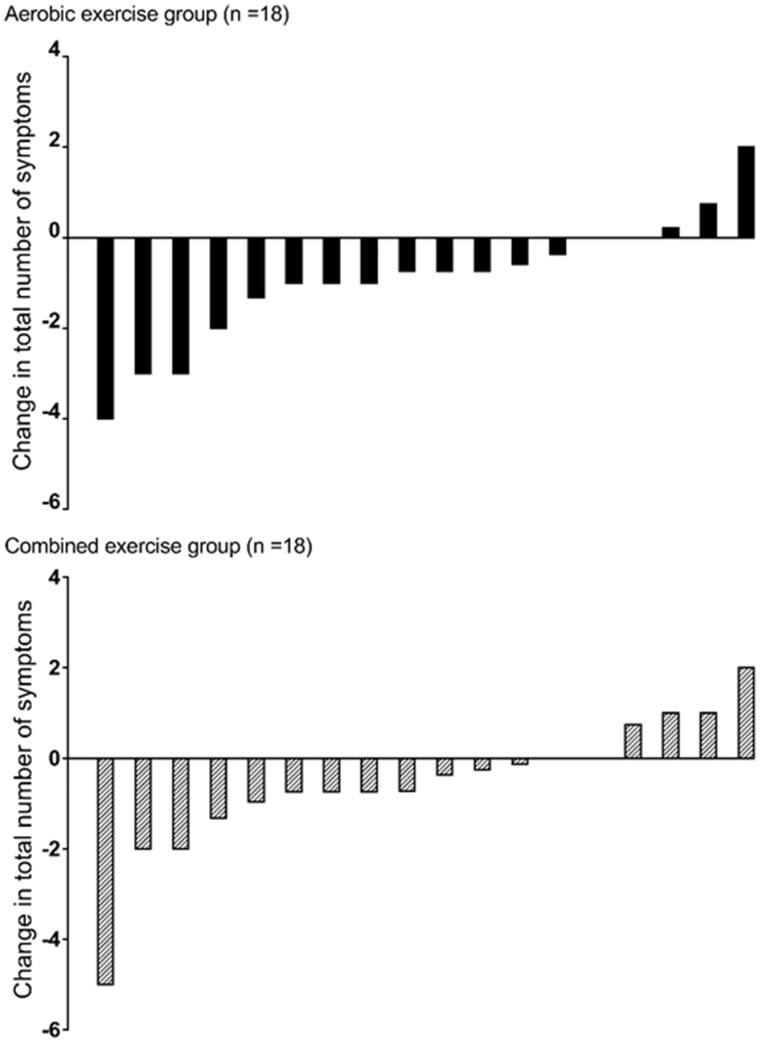
Thirty-six patients [mean ± SD 61.6 ± 11.8 years, 22 (61%) females, estimated glomerular filtration rate: 25.5 ± 7.8 mL/min/1.73 m] not requiring renal replacement therapy underwent 12 weeks (3 times/week) of supervised aerobic exercise (AE), or a combination (CE) of AE plus resistance training. Outcomes included self-reported symptom burden, fatigue, HRQoL and physical activity.
Exercise reduced the total number of symptoms reported by 17% and had favourable effects on fatigue in both groups. AE reduced the frequency of 'itching', 'impotence' and 'shortness of breath' symptoms, and the intrusiveness for symptoms of 'sleep disturbance', 'loss of muscular strength/power', 'muscle spasm/stiffness' and 'restless legs'. The addition of resistance exercise in the CE group saw a reduction in 'loss of muscular strength/power'. No changes were seen in subjective PF or physical activity levels. AE increased self-efficacy for physical activity.
Supervised exercise had favourable effects on symptom frequency and intrusiveness, including substantial improvements in fatigue. Although the intervention did not improve self-reported physical activity levels, AE increased patients' self-efficacy for physical activity. These favourable changes in self-reported outcomes support the important role of exercise in CKD.
慢性肾脏病(CKD)患者承受着较高的症状负担,包括疲劳、睡眠困难、肌肉无力和疼痛。这些症状会降低身体功能(PF)和活动水平,并导致健康相关生活质量(HRQoL)较差。尽管越来越多的证据表明运动后CKD患者会出现积极的生理变化,但其对自我报告的症状负担、疲劳、HRQoL和身体活动的影响证据有限。
36例[平均±标准差61.6±11.8岁,22例(61%)为女性,估计肾小球滤过率:25.5±7.8 mL/min/1.73 m²]不需要肾脏替代治疗的患者接受为期12周(每周3次)的有监督有氧运动(AE),或AE加抗阻训练的联合运动(CE)。结果包括自我报告的症状负担、疲劳、HRQoL和身体活动。
运动使报告的症状总数减少了17%,且两组在疲劳方面均有良好效果。AE减少了“瘙痒”“阳痿”和“呼吸急促”症状的发生频率,以及“睡眠障碍”“肌肉力量/功率丧失”“肌肉痉挛/僵硬”和“不宁腿”症状的侵扰性。CE组增加抗阻训练后,“肌肉力量/功率丧失”有所减少。主观PF或身体活动水平未见变化。AE提高了身体活动的自我效能感。
有监督的运动对症状频率和侵扰性有良好效果,包括疲劳的显著改善。尽管干预未改善自我报告的身体活动水平,但AE提高了患者身体活动自我效能感。这些自我报告结果的积极变化支持了运动在CKD中的重要作用。