Department of Surgery, School of Medicine, Keio University, 35 Shinanomachi, Shinjuku-ku, Tokyo, 160-8582, Japan.
Center for Endoscopy, Kawasaki Municipal Ida Hospital, Kawasaki, Japan.
World J Surg Oncol. 2019 Feb 13;17(1):32. doi: 10.1186/s12957-019-1571-2.
Endoscopic resection (ER) has come to be recognized as a standard treatment for early gastric cancer (EGC). While its adoption is expanding, ER remains restricted to cases of EGC without lymph node metastasis for the treatment of local resection. On the other hand, histopathological analyses of surgically resected specimens of EGC have revealed the presence of lymph node (LN) metastasis in some cases of mucosal gastric cancer (MGC) and undifferentiated MGC (UD-MGC) is considered to have higher risk of nodal metastases than differentiated MGC (D-MGC). To evaluate the risk factors for LN metastasis in MGC, we investigated the characteristics of UD-MGC associated with LN metastasis.
Among all UD-MGC patients who underwent surgery as initial treatment, between January 2000 and March 2016, we reviewed the clinicopathological data, including the preoperative endoscopic findings and histopathological findings in the resected specimens, of the 11 UD-MGC patients who were identified as having lymph node metastasis. Furthermore, in comparison with cases without lymph node metastasis, we examined the possibility of expansion of the indication for local treatment.
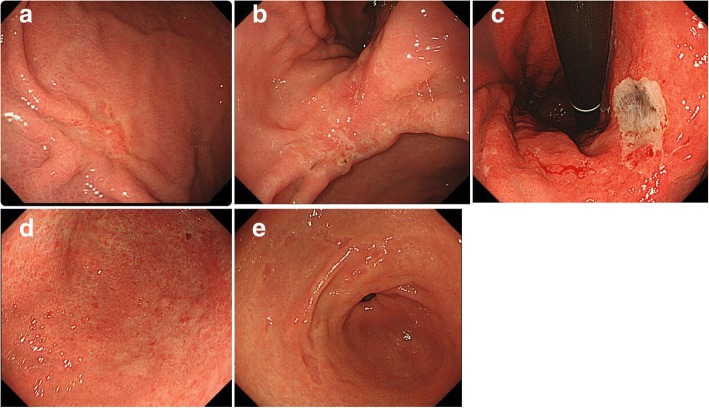
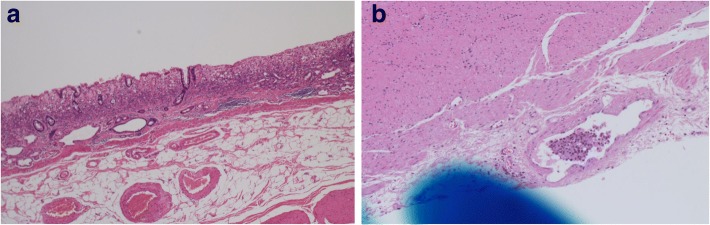
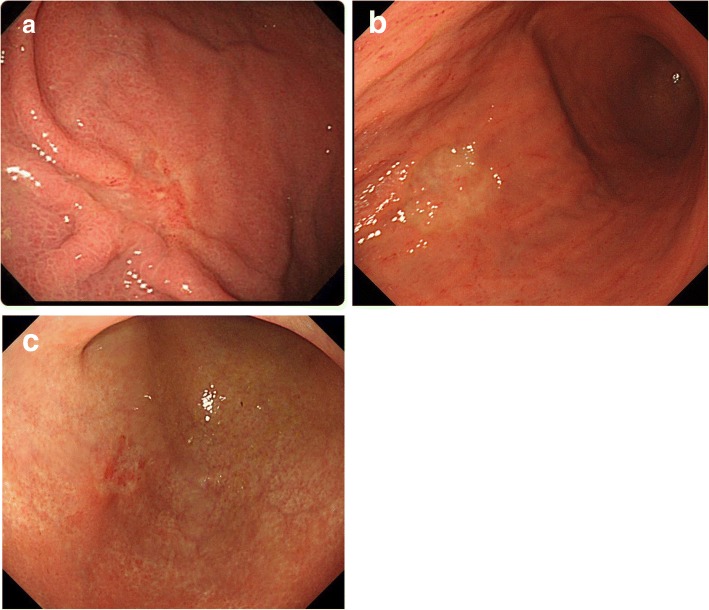
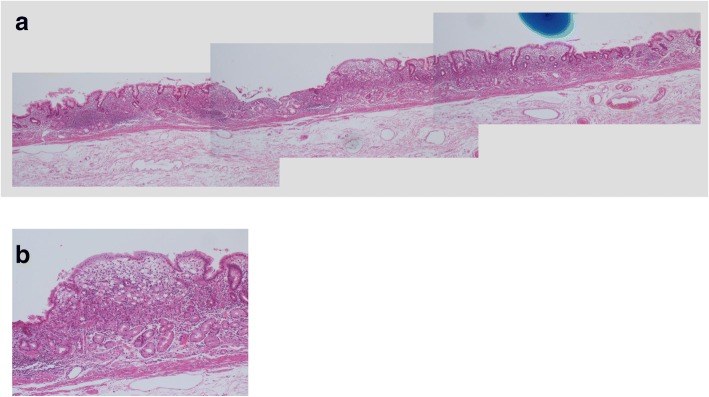
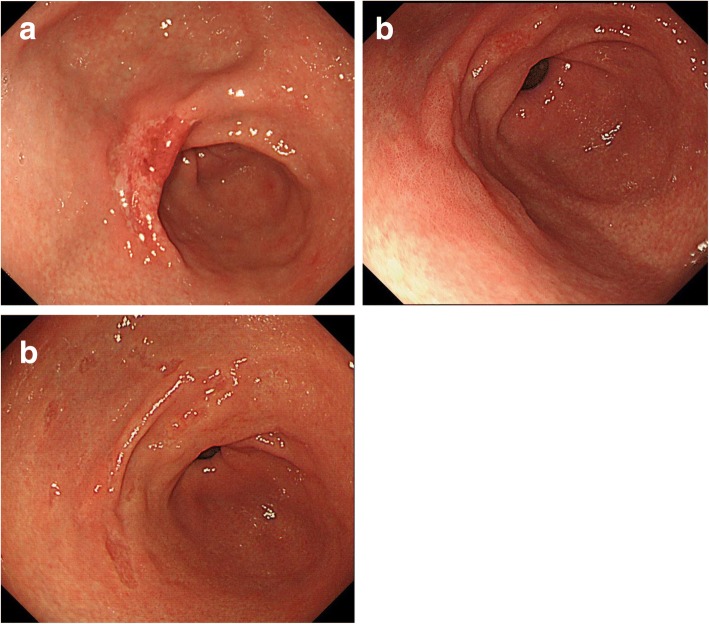
In most of the cases of UD-MGC with LN metastasis, the lesions were relatively large (> 20 mm in diameter) and of the clearly depressed type with faded color and apparent border, and histopathology revealed a high percentage of cases with lymphatic invasion and a predominance of signet ring cell carcinomas. No cases with LN metastasis without depressed macroscopic type nor signet ring cell carcinoma component existed. A degree of invasion of lamina propria (LP) or muscularis mucosae (MM) had same relation to the risk of LN metastasis.
In this study, none of the cases of undifferentiated-type mucosal cancer (UD-MGC) with LN metastasis satisfied the current adoption criteria for ER. We suggested significant risk factors for LN metastasis in UD-MGC cases as depressed tumor type, presence of a signet ring cell carcinoma component, presence of lymphatic tumor invasion, and a large tumor size. More detailed analyses of the endoscopic and histopathological findings may allow further risk classification for LN metastasis in cases of UD-MGC.
内镜下切除(ER)已被公认为治疗早期胃癌(EGC)的标准治疗方法。虽然它的应用正在扩大,但 ER 仍然仅限于没有淋巴结转移的 EGC 病例,用于局部切除治疗。另一方面,对手术切除的 EGC 标本的组织病理学分析显示,在一些黏膜胃癌(MGC)和未分化 MGC(UD-MGC)病例中存在淋巴结(LN)转移,并且认为 UD-MGC 比分化型 MGC(D-MGC)具有更高的淋巴结转移风险。为了评估 MGC 中 LN 转移的危险因素,我们研究了与 LN 转移相关的 UD-MGC 的特征。
在 2000 年 1 月至 2016 年 3 月期间,作为初始治疗接受手术的所有 UD-MGC 患者中,我们回顾了 11 例经病理证实存在淋巴结转移的 UD-MGC 患者的临床病理资料,包括术前内镜检查结果和手术标本的组织病理学检查结果。此外,与无淋巴结转移的病例相比,我们检查了扩大局部治疗适应证的可能性。
在大多数存在 LN 转移的 UD-MGC 病例中,病变相对较大(直径>20mm),呈明显凹陷型,颜色消退,边界明显,组织病理学显示淋巴管浸润和印戒细胞癌为主的病例比例较高。不存在无凹陷型大体类型或印戒细胞癌成分的 LN 转移病例。固有层(LP)或黏膜肌层(MM)的侵犯程度与 LN 转移的风险有关。
在这项研究中,没有一例存在 LN 转移的未分化型黏膜癌(UD-MGC)符合 ER 的当前采用标准。我们提出了 UD-MGC 病例中 LN 转移的显著危险因素,包括凹陷型肿瘤类型、存在印戒细胞癌成分、存在淋巴管肿瘤浸润和肿瘤较大。对内镜和组织病理学发现的更详细分析可能允许进一步对 UD-MGC 病例的 LN 转移进行风险分类。