Toyoshima Osamu, Nishizawa Toshihiro, Yoshida Shuntaro, Aoki Tomonori, Nagura Fumiko, Sakitani Kosuke, Tsuji Yosuke, Nakagawa Hayato, Suzuki Hidekazu, Koike Kazuhiko
Department of Gastroenterology, Toyoshima Endoscopy Clinic, Tokyo 157-0066, Japan.
Department of Gastroenterology, Graduate School of Medicine, The University of Tokyo, Tokyo 113-8655, Japan.
World J Gastrointest Endosc. 2021 May 16;13(5):125-136. doi: 10.4253/wjge.v13.i5.125.
Gastric cancers can be categorized into diffuse- and intestinal-type cancers based on the Lauren histopathological classification. These two subtypes show distinct differences in metastasis frequency, treatment application, and prognosis. Therefore, accurately assessing the Lauren classification before treatment is crucial. However, studies on the gastritis endoscopy-based Kyoto classification have recently shown that endoscopic diagnosis has improved.
To investigate patient characteristics including endoscopic gastritis associated with diffuse- and intestinal-type gastric cancers in ()-infected patients.
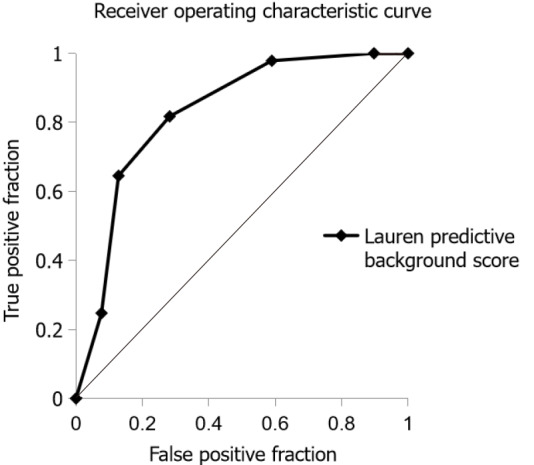
Patients who underwent esophagogastroduodenoscopy at the Toyoshima Endoscopy Clinic were enrolled. The Kyoto classification included atrophy, intestinal metaplasia, enlarged folds, nodularity, and diffuse redness. The effects of age, sex, and Kyoto classification score on gastric cancer according to the Lauren classification were analyzed. We developed the Lauren predictive background score based on the coefficients of a logistic regression model using variables independently associated with the Lauren classification. Area under the receiver operative characteristic curve and diagnostic accuracy of this score were examined.
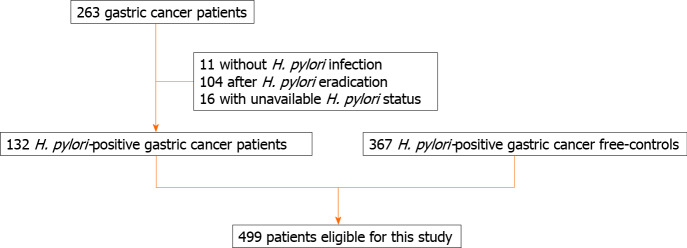
A total of 499 -infected patients (49.6% males; average age: 54.9 years) were enrolled; 132 patients with gastric cancer (39 diffuse- and 93 intestinal-type cancers) and 367 cancer-free controls were eligible. Gastric cancer was independently associated with age ≥ 65 years, high atrophy score, high intestinal metaplasia score, and low nodularity score when compared to the control. Factors independently associated with intestinal-type cancer were age ≥ 65 years (coefficient: 1.98), male sex (coefficient: 1.02), high intestinal metaplasia score (coefficient: 0.68), and low enlarged folds score (coefficient: -1.31) when compared to diffuse-type cancer. The Lauren predictive background score was defined as the sum of +2 (age ≥ 65 years), +1 (male sex), +1 (endoscopic intestinal metaplasia), and -1 (endoscopic enlarged folds) points. Area under the receiver operative characteristic curve of the Lauren predictive background score was 0.828 for predicting intestinal-type cancer. With a cut-off value of +2, the sensitivity, specificity, and accuracy of the Lauren predictive background score were 81.7%, 71.8%, and 78.8%, respectively.
Patient backgrounds, such as age, sex, endoscopic intestinal metaplasia, and endoscopic enlarged folds are useful for predicting the Lauren type of gastric cancer.
根据劳伦组织病理学分类,胃癌可分为弥漫型和肠型癌。这两种亚型在转移频率、治疗应用和预后方面表现出明显差异。因此,在治疗前准确评估劳伦分类至关重要。然而,最近关于基于胃炎内镜检查的京都分类的研究表明,内镜诊断有所改善。
调查()感染患者中与弥漫型和肠型胃癌相关的内镜下胃炎等患者特征。
纳入在丰岛内镜诊所接受食管胃十二指肠镜检查的患者。京都分类包括萎缩、肠化生、皱襞增大、结节状和弥漫性发红。分析年龄、性别和京都分类评分对根据劳伦分类的胃癌的影响。我们基于使用与劳伦分类独立相关的变量的逻辑回归模型的系数开发了劳伦预测背景评分。检查该评分的受试者操作特征曲线下面积和诊断准确性。
共纳入499例()感染患者(男性占49.6%;平均年龄:54.9岁);132例胃癌患者(39例弥漫型和93例肠型癌)和367例无癌对照符合条件。与对照组相比,胃癌与年龄≥65岁、高萎缩评分、高肠化生评分和低结节状评分独立相关。与弥漫型癌相比,与肠型癌独立相关的因素为年龄≥65岁(系数:1.98)、男性(系数:1.02)、高肠化生评分(系数:0.68)和低皱襞增大评分(系数:-1.31)。劳伦预测背景评分定义为+2分(年龄≥65岁)、+1分(男性)、+1分(内镜下肠化生)和-1分(内镜下皱襞增大)的总和。劳伦预测背景评分预测肠型癌的受试者操作特征曲线下面积为0.828。截断值为+2时,劳伦预测背景评分的敏感性、特异性和准确性分别为81.7%、71.8%和78.8%。
年龄、性别、内镜下肠化生和内镜下皱襞增大等患者背景有助于预测胃癌的劳伦类型。