Kim Danbi, Shin Ju Ae, Han Seung Beom, Chung Nack-Gyun, Jeong Dae Chul
Department of Pediatrics.
The Vaccine Bio Research Institute.
Medicine (Baltimore). 2019 Feb;98(7):e14559. doi: 10.1097/MD.0000000000014559.
Pneumocystis jirovecii causes severe pneumonia in immunocompromised hosts. Human immunodeficiency virus infection, malignancy, solid organ or hematopoietic cell transplantation, and primary immune deficiency compose the risk factors for Pneumocystis pneumonia (PCP) in children, and PCP can be an initial clinical manifestation of primary immune deficiency.
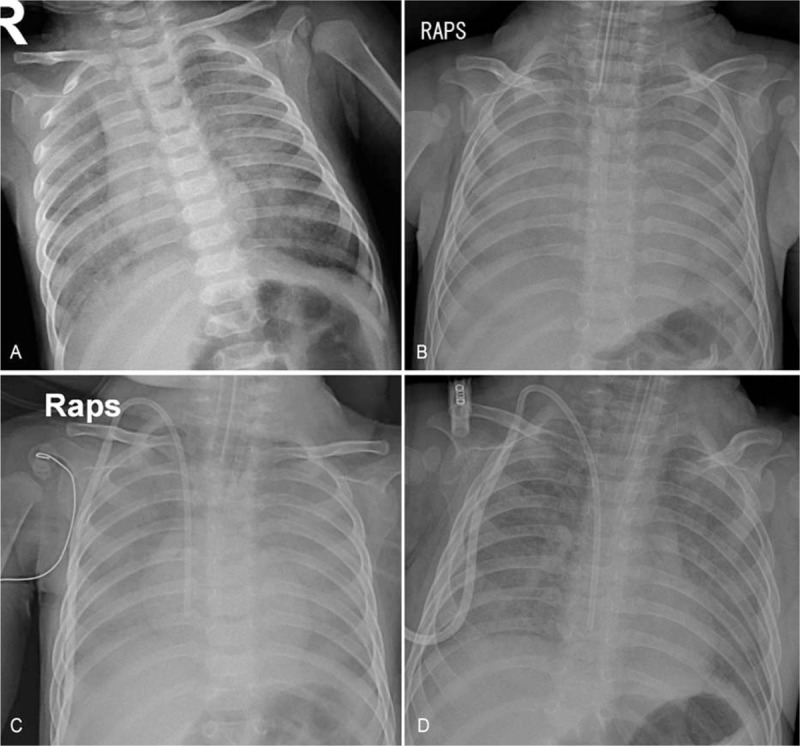
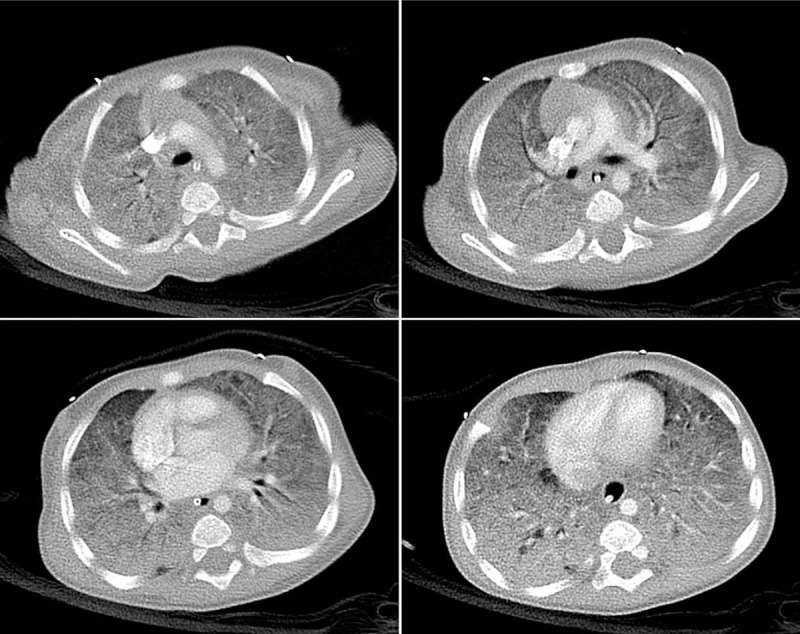
A 5-month-old infant presented with cyanosis and tachypnea. He had no previous medical or birth history suggesting primary immune deficiency. He was diagnosed with interstitial pneumonia on admission.
He was diagnosed with PCP, and further evaluations revealed underlying X-linked hyper-IgM syndrome.
He was treated with trimethoprim/sulfamethoxazole for PCP, and eventually received allogeneic hematopoietic cell transplantation for hyper-IgM syndrome.
Twenty months have passed after transplantation without severe complications.
PCP should be considered in infants presenting with severe interstitial pneumonia even in the absence of evidence of immune deficiency. Primary immune deficiency should also be suspected in infants diagnosed with PCP.
耶氏肺孢子菌可在免疫功能低下的宿主中引起严重肺炎。人类免疫缺陷病毒感染、恶性肿瘤、实体器官或造血细胞移植以及原发性免疫缺陷构成儿童肺孢子菌肺炎(PCP)的危险因素,且PCP可能是原发性免疫缺陷的初始临床表现。
一名5个月大的婴儿出现发绀和呼吸急促。他既往无提示原发性免疫缺陷的病史或出生史。入院时被诊断为间质性肺炎。
他被诊断为PCP,进一步评估发现潜在的X连锁高IgM综合征。
他接受了甲氧苄啶/磺胺甲恶唑治疗PCP,最终因高IgM综合征接受了异基因造血细胞移植。
移植后已过去20个月,无严重并发症。
即使在没有免疫缺陷证据的情况下,对于出现严重间质性肺炎的婴儿也应考虑PCP。对于诊断为PCP的婴儿也应怀疑原发性免疫缺陷。