Department of Clinical Pharmacy, University Medical Center Utrecht, Utrecht, the Netherlands.
Department of Neonatology, Wilhelmina Children's Hospital, University Medical Center Utrecht, Utrecht, the Netherlands.
PLoS One. 2019 Feb 14;14(2):e0211910. doi: 10.1371/journal.pone.0211910. eCollection 2019.
Morphine is a commonly used drug in encephalopathic neonates treated with therapeutic hypothermia after perinatal asphyxia. Pharmacokinetics and optimal dosing of morphine in this population are largely unknown. The objective of this study was to describe pharmacokinetics of morphine and its metabolites morphine-3-glucuronide and morphine-6-glucuronide in encephalopathic neonates treated with therapeutic hypothermia and to develop pharmacokinetics based dosing guidelines for this population.
Term and near-term encephalopathic neonates treated with therapeutic hypothermia and receiving morphine were included in two multicenter cohort studies between 2008-2010 (SHIVER) and 2010-2014 (PharmaCool). Data were collected during hypothermia and rewarming, including blood samples for quantification of morphine and its metabolites. Parental informed consent was obtained for all participants.
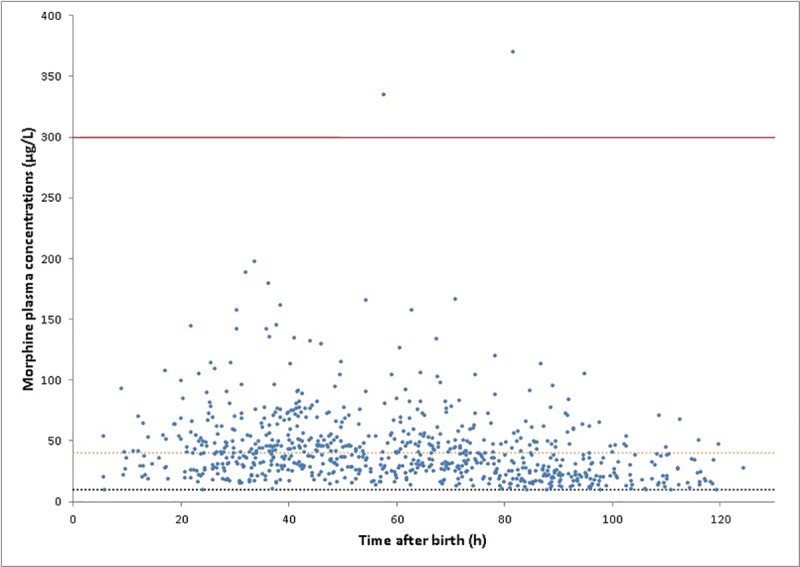
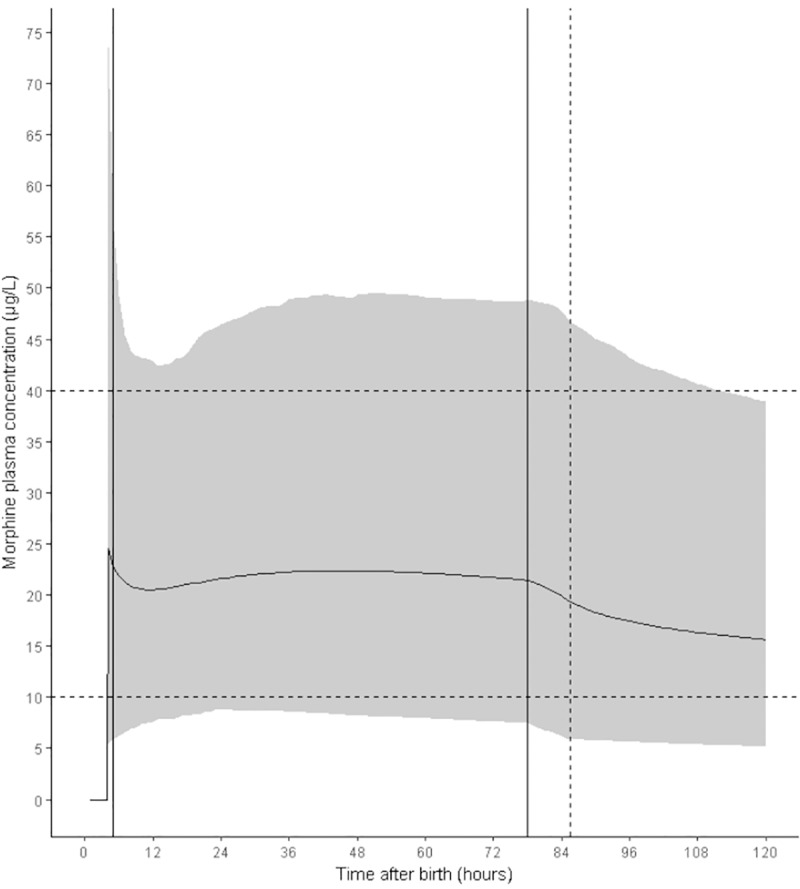
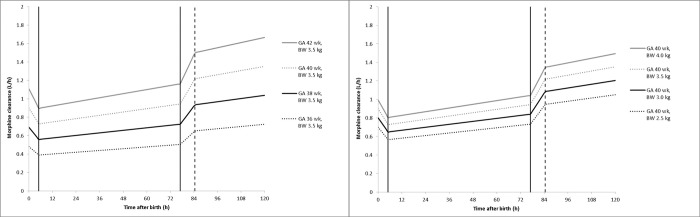
244 patients (GA mean (sd) 39.8 (1.6) weeks, BW mean (sd) 3,428 (613) g, male 61.5%) were included. Morphine clearance was reduced under hypothermia (33.5°C) by 6.89%/°C (95% CI 5.37%/°C- 8.41%/°C, p<0.001) and metabolite clearance by 4.91%/°C (95% CI 3.53%/°C- 6.22%/°C, p<0.001) compared to normothermia (36.5°C). Simulations showed that a loading dose of 50 μg/kg followed by continuous infusion of 5 μg/kg/h resulted in morphine plasma concentrations in the desired range (between 10 and 40 μg/L) during hypothermia.
Clearance of morphine and its metabolites in neonates is affected by therapeutic hypothermia. The regimen suggested by the simulations will be sufficient in the majority of patients. However, due to the large interpatient variability a higher dose might be necessary in individual patients to achieve the desired effect.
www.trialregister.nl NTR2529.
在接受围产期窒息后治疗性低温治疗的脑病新生儿中,吗啡是一种常用的药物。该药在该人群中的药代动力学和最佳剂量尚不清楚。本研究的目的是描述接受治疗性低温治疗的脑病新生儿中吗啡及其代谢物吗啡-3-葡萄糖醛酸苷和吗啡-6-葡萄糖醛酸苷的药代动力学,并为该人群制定基于药代动力学的给药指南。
2008-2010 年(SHIVER)和 2010-2014 年(PharmaCool)期间,在接受治疗性低温治疗并接受吗啡治疗的足月和近足月脑病新生儿中进行了两项多中心队列研究,将这些新生儿纳入其中。在低温和复温期间收集数据,包括用于定量测定吗啡及其代谢物的血样。所有参与者均获得了父母的知情同意。
共纳入 244 例患者(GA 均值(标准差)39.8(1.6)周,BW 均值(标准差)3428(613)g,男性 61.5%)。与正常体温(36.5°C)相比,低温(33.5°C)下吗啡清除率降低 6.89%/°C(95%CI 5.37%/°C-8.41%/°C,p<0.001),代谢物清除率降低 4.91%/°C(95%CI 3.53%/°C-6.22%/°C,p<0.001)。模拟结果表明,50μg/kg 的负荷剂量后,以 5μg/kg/h 的速度持续输注,可使吗啡在低温下的血浆浓度在理想范围内(10-40μg/L 之间)。
新生儿吗啡及其代谢物的清除受治疗性低温的影响。模拟建议的方案在大多数患者中是足够的。然而,由于个体间的变异性很大,为了达到预期的效果,个别患者可能需要更高的剂量。
www.trialregister.nl NTR2529。