Department of Radiation Oncology, Mayo Clinic, Rochester, Minnesota, United States of America.
PLoS One. 2019 Feb 14;14(2):e0212412. doi: 10.1371/journal.pone.0212412. eCollection 2019.
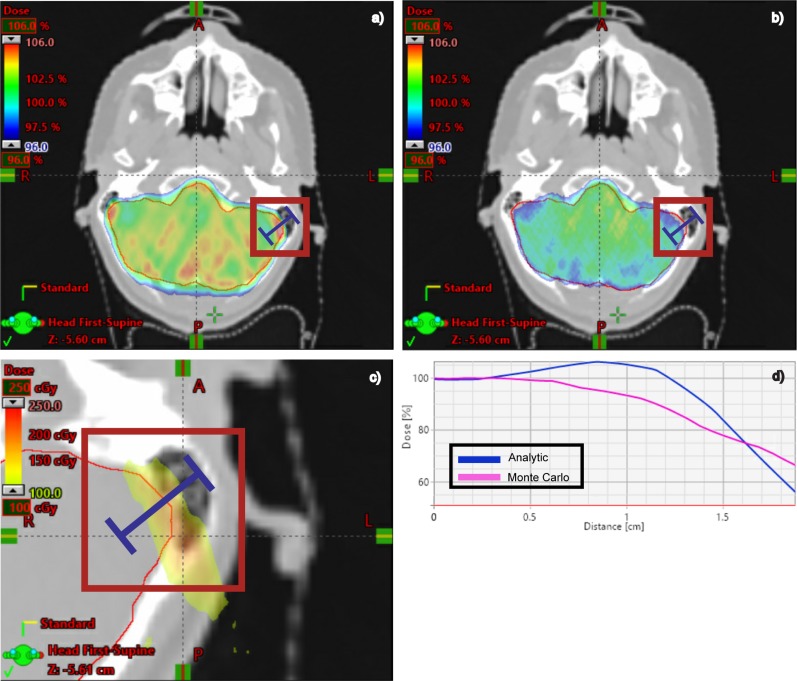
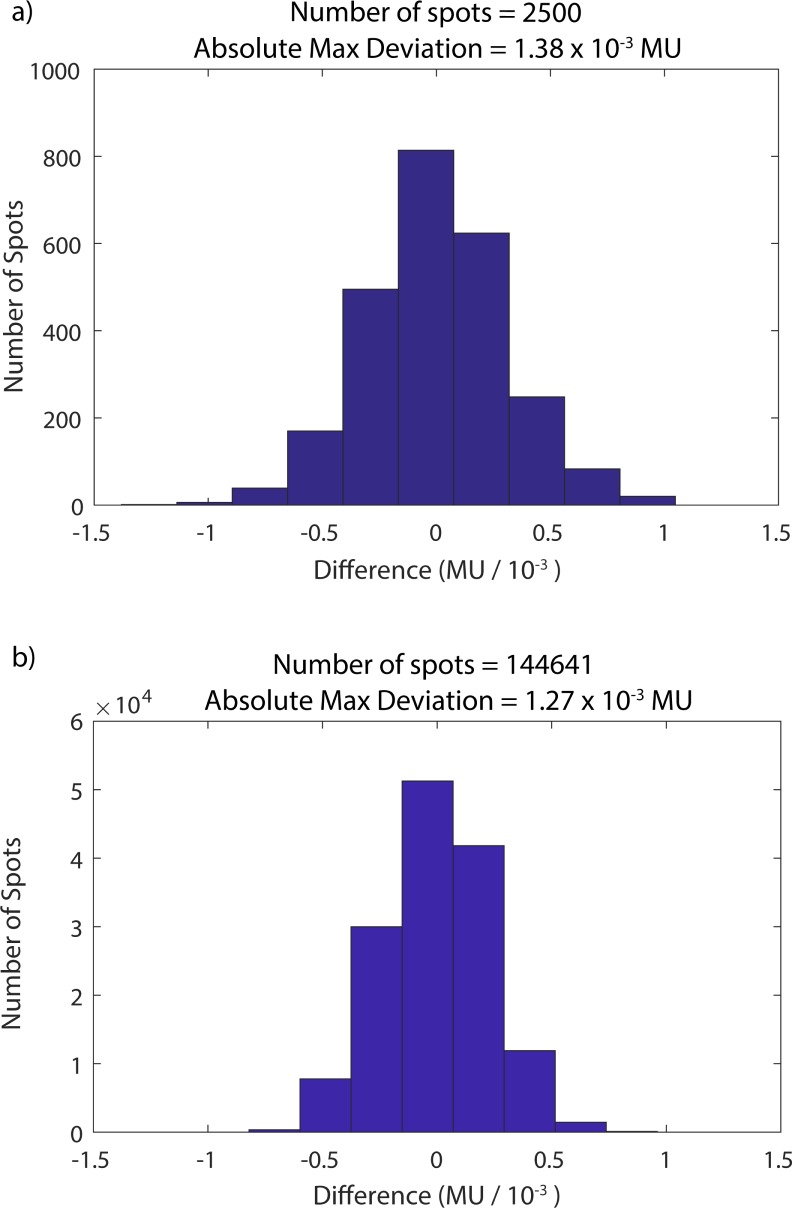
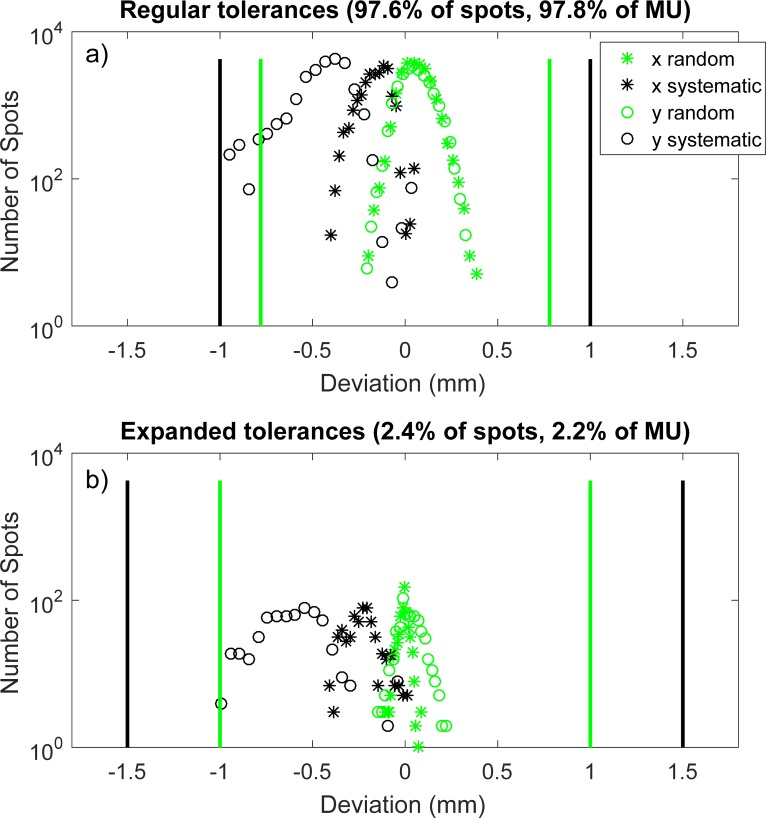
The purpose of this work was to develop an end-to-end patient-specific quality assurance (QA) technique for spot-scanned proton therapy that is more sensitive and efficient than traditional approaches. The patient-specific methodology relies on independently verifying the accuracy of the delivered proton fluence and the dose calculation in the heterogeneous patient volume. A Monte Carlo dose calculation engine, which was developed in-house, recalculates a planned dose distribution on the patient CT data set to verify the dose distribution represented by the treatment planning system. The plan is then delivered in a pre-treatment setting and logs of spot position and dose monitors, which are integrated into the treatment nozzle, are recorded. A computational routine compares the delivery log to the DICOM spot map used by the Monte Carlo calculation to ensure that the delivered parameters at the machine match the calculated plan. Measurements of dose planes using independent detector arrays, which historically are the standard approach to patient-specific QA, are not performed for every patient. The nozzle-integrated detectors are rigorously validated using independent detectors in regular QA intervals. The measured data are compared to the expected delivery patterns. The dose monitor reading deviations are reported in a histogram, while the spot position discrepancies are plotted vs. spot number to facilitate independent analysis of both random and systematic deviations. Action thresholds are linked to accuracy of the commissioned delivery system. Even when plan delivery is acceptable, the Monte Carlo second check system has identified dose calculation issues which would not have been illuminated using traditional, phantom-based measurement techniques. The efficiency and sensitivity of our patient-specific QA program has been improved by implementing a procedure which independently verifies patient dose calculation accuracy and plan delivery fidelity. Such an approach to QA requires holistic integration and maintenance of patient-specific and patient-independent QA.
这项工作的目的是开发一种端到端的质子治疗患者特异性质量保证(QA)技术,该技术比传统方法更敏感、更高效。患者特异性方法依赖于独立验证交付质子通量的准确性和在异质患者体积中的剂量计算。一个内部开发的蒙特卡罗剂量计算引擎重新计算患者 CT 数据集上的计划剂量分布,以验证治疗计划系统表示的剂量分布。然后在治疗前设置中交付计划,并记录集成到治疗喷嘴中的点位置和剂量监测器的日志。一个计算例程将交付日志与蒙特卡罗计算中使用的 DICOM 点图进行比较,以确保机器上的交付参数与计算计划匹配。使用独立探测器阵列测量剂量平面的方法,从历史上看,这是患者特异性 QA 的标准方法,不会对每个患者进行。在常规 QA 间隔中使用独立探测器对喷嘴集成探测器进行严格验证。将测量数据与预期的输送模式进行比较。剂量监测器读数偏差以直方图形式报告,而点位置差异则以点号绘制,以方便对随机和系统偏差进行独立分析。动作阈值与委托输送系统的准确性相关联。即使计划输送是可接受的,蒙特卡罗二次检查系统也已经确定了剂量计算问题,如果使用传统的、基于体模的测量技术,这些问题将不会被揭示出来。通过实施一种独立验证患者剂量计算准确性和计划输送保真度的程序,提高了我们患者特异性 QA 程序的效率和敏感性。这种 QA 方法需要对患者特异性和患者非特异性 QA 进行整体集成和维护。