Zvitambo Institute for Maternal and Child Health Research, Harare, Zimbabwe.
Centre for Genomics and Child Health, Blizard Institute, Queen Mary University of London, United Kingdom.
Clin Infect Dis. 2019 Nov 27;69(12):2074-2081. doi: 10.1093/cid/ciz140.
Oral vaccines have lower efficacy in developing compared to developed countries. Poor water, sanitation, and hygiene (WASH) may contribute to reduced oral vaccine immunogenicity.
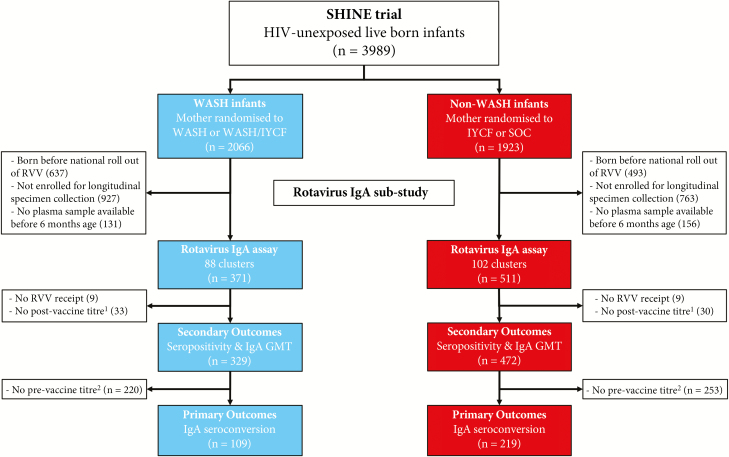
We conducted a cluster-randomized 2 × 2 factorial trial in rural Zimbabwe. Pregnant women and their infants were eligible if they lived in clusters randomized to (1) standard of care (52 clusters); (2) improved infant feeding (53 clusters); (3) WASH: ventilated improved pit latrine, 2 hand-washing stations, liquid soap, chlorine, infant play space, and hygiene counseling (53 clusters); or (4) feeding plus WASH (53 clusters). This substudy compared oral rotavirus vaccine (RVV) seroconversion (primary outcome), and seropositivity and geometric mean titer (GMT) (secondary outcomes), in WASH vs non-WASH infants by intention-to-treat analysis.
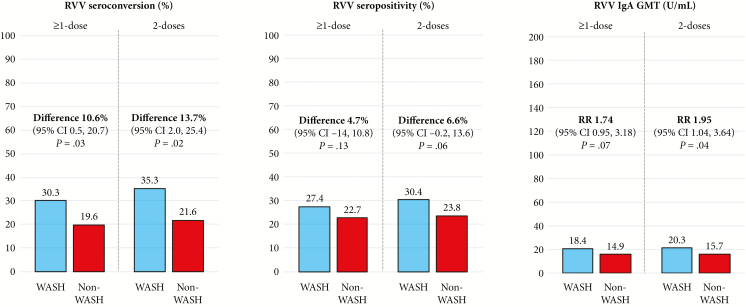
We included 801 infants with documented RVV receipt and postvaccine titer measurements (329 from 84 WASH clusters; 472 from 102 non-WASH clusters); 328 infants with prevaccination titers were included in the primary outcome. Thirty-three of 109 (30.3%) infants in the WASH group seroconverted following rotavirus vaccination, compared to 43 of 219 (19.6%) in the non-WASH group (absolute difference, 10.6% [95% confidence interval {CI}, .54%-20.7%]; P = .031). In the WASH vs non-WASH groups, 90 of 329 (27.4%) vs 107 of 472 (22.7%) were seropositive postvaccination (absolute difference, 4.7% [95% CI, -1.4% to 10.8%]; P = .130), and antirotavirus GMT was 18.4 (95% CI, 15.6-21.7) U/mL vs 14.9 (95% CI, 13.2-16.8) U/mL (P = .072).
Improvements in household WASH led to modest but significant increases in seroconversion to RVV in rural Zimbabwean infants.
NCT01824940.
与发达国家相比,发展中国家口服疫苗的效果较低。较差的水、环境卫生和个人卫生(WASH)条件可能会降低口服疫苗的免疫原性。
我们在津巴布韦农村地区开展了一项集群随机 2×2 析因试验。如果孕妇及其婴儿居住在随机分配到以下 4 个组的集群中,则符合纳入条件:(1)标准护理(52 个集群);(2)改善婴儿喂养(53 个集群);(3)WASH:通风改良坑式厕所、2 个洗手站、液体肥皂、氯、婴儿游乐空间和卫生咨询(53 个集群);或(4)喂养加 WASH(53 个集群)。这项亚研究通过意向治疗分析比较了 WASH 组与非 WASH 组婴儿的口服轮状病毒疫苗(RVV)血清转化率(主要结局)以及血清阳性率和几何平均滴度(GMT)(次要结局)。
我们纳入了 801 名接受 RVV 疫苗接种并有疫苗接种后滴度检测记录的婴儿(84 个 WASH 集群中有 329 名婴儿,102 个非 WASH 集群中有 472 名婴儿);在主要结局中,328 名婴儿有疫苗接种前滴度数据。接种 RVV 后,33 名(30.3%)WASH 组婴儿发生血清转化率,而非 WASH 组有 43 名(19.6%)婴儿发生血清转化率(绝对差异,10.6%[95%置信区间{CI}:.54%-20.7%];P=.031)。在 WASH 组与非 WASH 组中,接种后血清阳性率分别为 90 名(27.4%)和 107 名(22.7%)(绝对差异,4.7%[95%CI:-1.4%至 10.8%];P=.130),抗轮状病毒 GMT 分别为 18.4(95%CI:15.6-21.7)U/mL 和 14.9(95%CI:13.2-16.8)U/mL(P=.072)。
津巴布韦农村地区家庭 WASH 条件的改善导致了农村地区婴儿对 RVV 的血清转化率适度但显著增加。
NCT01824940。