Division of Pediatric Hematology/Oncology, Department of Pediatrics, Weill Cornell Medicine, New York, New York.
Department of Medicine, Michael G. DeGroote School of Medicine, McMaster University, and McMaster Centre for Transfusion Research, Hamilton Health Sciences, Hamilton, Ontario, Canada.
Am J Hematol. 2019 May;94(5):546-553. doi: 10.1002/ajh.25444. Epub 2019 Mar 13.
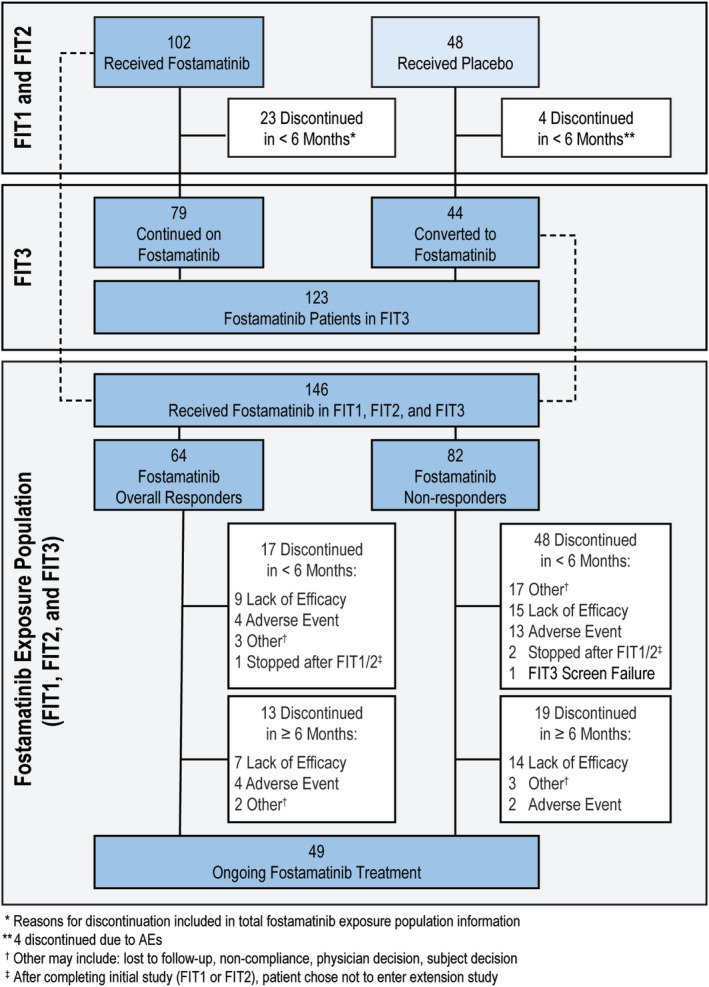
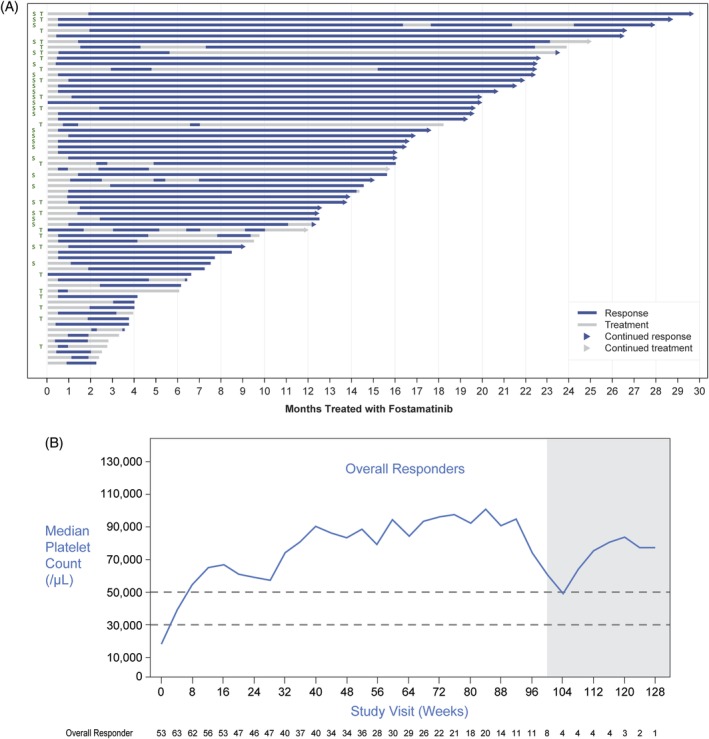
Two randomized, double-blind, placebo-controlled studies demonstrated responses (≥50 000/μL) to fostamatinib in adults with long-standing immune thrombocytopenia (ITP). The long-term safety and efficacy of fostamatinib were evaluated in a follow-on, open-label extension (OLE) study. Patients received double-blind fostamatinib in the randomized trials, and responders continued the same dose, 100 to 150 mg BID, in the OLE study. Nonresponders received 100 mg BID for 4 weeks and could escalate to 150 mg BID at week 4. Endpoints included stable response, platelet count ≥50 000/μL at 4/6 biweekly (randomized trials) or 2/3 monthly visits (OLE), and overall response, ≥1 platelet count ≥50 000/μL during weeks 1 to 12. A total of 146 patients received fostamatinib including 123 in the OLE study. Median treatment duration was 6.7 months. Baseline median ITP duration was 8 years and median platelet count was 16 000/μL; prior treatments included thrombopoietic (TPO) agents (47%), splenectomy (35%), and rituximab (32%). Twenty-seven (18%) patients achieved a stable response with median duration of >28 months and a median platelet count of 89 000/μL. Sixty-four (44%) patients achieved an overall response (including stable responders) with a median platelet count of 63 000/μL and a median response duration of >28 months. Twenty-four of 71 (34%) patients who had failed TPO agents achieved overall responses to fostamatinib. The most common adverse events (AEs) were diarrhea, hypertension, nausea, epistaxis, and abnormal liver function tests. Most AEs were mild/moderate and resolved or were managed with dose reduction, dose interruption, and/or secondary medication. Almost half of the patients achieved an overall response, and most of these maintained their responses for >2 years. No new or increased frequency of AEs was seen at up to 31 months of treatment.
两项随机、双盲、安慰剂对照研究显示,在患有长期免疫性血小板减少症(ITP)的成年人中,福他替尼有应答(≥50,000/μL)。福他替尼的长期安全性和疗效在一项后续的开放标签扩展(OLE)研究中进行了评估。在随机试验中,患者接受双盲福他替尼治疗,在 OLE 研究中,应答者继续使用相同剂量(100-150mg,bid)。无应答者接受 100mg,bid 治疗 4 周,可在第 4 周时升级为 150mg,bid。终点包括稳定应答(在随机试验中为第 4/6 双周或 OLE 研究中的第 2/3 个月访视时血小板计数≥50,000/μL)、血小板计数≥50,000/μL(在第 1 至 12 周)≥1 的总应答。共有 146 名患者接受福他替尼治疗,其中 123 名患者进入 OLE 研究。中位治疗持续时间为 6.7 个月。基线时 ITP 持续时间中位数为 8 年,血小板计数中位数为 16,000/μL;既往治疗包括促血小板生成素(TPO)制剂(47%)、脾切除术(35%)和利妥昔单抗(32%)。27 名(18%)患者获得稳定应答,中位持续时间>28 个月,血小板计数中位数为 89,000/μL。64 名(44%)患者获得总应答(包括稳定应答者),血小板计数中位数为 63,000/μL,中位应答持续时间>28 个月。24 名曾接受 TPO 制剂治疗失败的患者对福他替尼有总体应答。最常见的不良事件(AE)是腹泻、高血压、恶心、鼻出血和肝功能异常。大多数 AE 为轻度/中度,经剂量降低、剂量中断和/或辅助药物治疗后缓解或得到控制。71 名患者中有 24 名(34%)接受 TPO 制剂治疗失败的患者获得了总体应答。大多数患者的应答持续时间>2 年。在长达 31 个月的治疗中,未观察到新的或增加的 AE 频率。