Makerere University Lung Institute & Division of Pulmonary Medicine, Department of Medicine, Makerere University College of Health Sciences, Kampala, Uganda.
GRIAC-Primary Care, department of General Practice and Elderly Care, University of Groningen, University Medical Center Groningen (UMCG), Groningen, The Netherlands.
BMC Public Health. 2019 Feb 22;19(1):227. doi: 10.1186/s12889-019-6562-2.
Recent large-scale population data on the prevalence of asthma and its risk factors are lacking in Uganda. This survey was conducted to address this data gap.
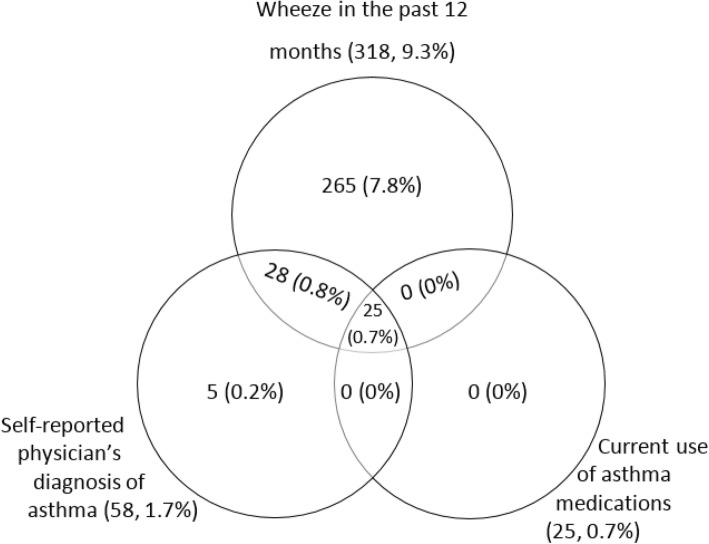
A general population based survey was conducted among people ≥12 years. A questionnaire was used to collect participants socio-demographics, respiratory symptoms, medical history, and known asthma risk factors. Participants who reported wheeze in the past 12 months, a physician diagnosis of asthma or current use of asthma medications were classified as having asthma. Asthmatics who were ≥ 35 years underwent spirometry to determine how many had fixed airflow obstruction (i.e. post bronchodilator forced expiratory volume in one second/forced vital capacity (FEV/FVC) ratio < lower limit of normal (LLN). Descriptive statistics were used to summarize participants' characteristics. Prevalence of asthma was calculated as a proportion of asthmatics over total survey population. To obtain factors independently associated with asthma, a random-effects model was fitted to the data.
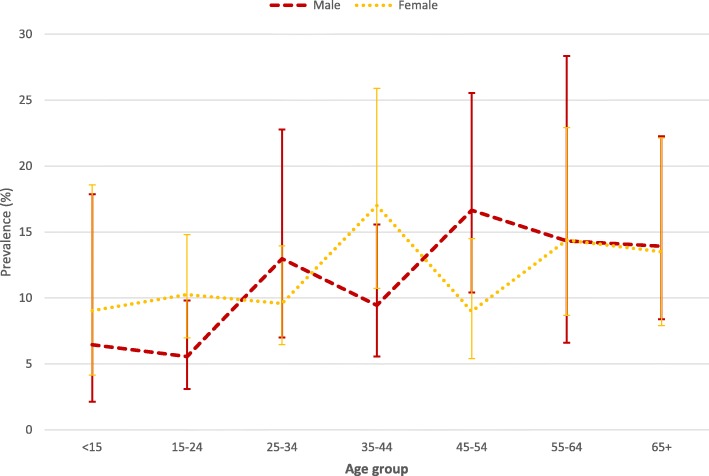
Of the 3416 participants surveyed, 61.2% (2088) were female, median age was 30 years (IQR, 20-45) and 323 were found to have asthma. Sixteen people with asthma ≥35 years had fixed airflow obstruction. The prevalence of asthma was 11.0% (95% CI:8.9-13.2; males 10.3%, females 11.4%, urban 13.0% and rural 8.9%. Significantly more people with asthma smoked than non-asthmatics: 14.2% vs. 6.3%, p < 0.001, were exposed to biomass smoke: 28.0% vs. 20.0%, p < 0.001, had family history of asthma: 26.9% vs. 9.4%, p, < 0.001, had history of TB: 3.1% vs. 1.30%, p = 0.01, and had hypertension: 17.9% vs. 12.0%, p = 0. 003. In multivariate analysis smoking, (adjusted odds ratio (AOR), 3.26 (1.96-5.41, p < 0.001) family history of asthma, AOR 2.90 (98-4.22 p- < 0.001), nasal congestion, AOR 3.56 (2.51-5.06, p < 0.001), biomass smoke exposure, AOR 2.04 (1.29-3.21, p = 0.002) and urban residence, AOR 2.01(1.23-3.27, p = 0.005) were independently associated with asthma.
Asthma is common in Uganda and is associated with smoking, biomass smoke exposure, urbanization, and allergic diseases. Health care systems should be strengthened to provide asthma care. Measures to reduce exposure to the identified associated factors are needed.
乌干达缺乏关于哮喘患病率及其危险因素的大规模人群数据。本调查旨在填补这一数据空白。
对≥12 岁的人群进行了一项基于人群的调查。使用问卷收集参与者的社会人口统计学、呼吸症状、病史和已知的哮喘危险因素。报告在过去 12 个月内有喘息、医生诊断为哮喘或当前使用哮喘药物的患者被归类为患有哮喘。≥35 岁的哮喘患者接受了肺量测定以确定有多少人存在固定气流阻塞(即支气管扩张剂后一秒用力呼气量/用力肺活量(FEV/FVC)比值<正常下限(LLN)。使用描述性统计来总结参与者的特征。哮喘的患病率计算为哮喘患者总数与总调查人群的比例。为了确定与哮喘独立相关的因素,使用随机效应模型对数据进行拟合。
在 3416 名接受调查的参与者中,61.2%(2088 人)为女性,中位年龄为 30 岁(IQR,20-45),发现 323 人患有哮喘。16 名≥35 岁的哮喘患者存在固定气流阻塞。哮喘的患病率为 11.0%(95%CI:8.9-13.2;男性 10.3%,女性 11.4%,城市 13.0%,农村 8.9%)。哮喘患者的吸烟率明显高于非哮喘患者:14.2%对 6.3%,p<0.001,暴露于生物质烟雾的比例为 28.0%对 20.0%,p<0.001,有哮喘家族史的比例为 26.9%对 9.4%,p<0.001,有结核病史的比例为 3.1%对 1.30%,p=0.01,有高血压的比例为 17.9%对 12.0%,p=0.003。在多变量分析中,吸烟(调整后的优势比(AOR),3.26(1.96-5.41,p<0.001),哮喘家族史,AOR 2.90(98-4.22,p<0.001),鼻塞,AOR 3.56(2.51-5.06,p<0.001),生物质烟雾暴露,AOR 2.04(1.29-3.21,p=0.002)和城市居住,AOR 2.01(1.23-3.27,p=0.005)与哮喘独立相关。
哮喘在乌干达很常见,与吸烟、生物质烟雾暴露、城市化和过敏性疾病有关。应加强卫生保健系统以提供哮喘护理。需要采取措施减少与已确定的相关因素的接触。