Department of Radiology, Severance Hospital, Research Institute of Radiological Science and Center for Clinical Imaging Data Science, Yonsei University College of Medicine, Seoul, Korea.
Department of Internal Medicine, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
Korean J Radiol. 2019 Mar;20(3):449-458. doi: 10.3348/kjr.2018.0469.
To identify an imaging predictor for the assessment of early treatment response to yttrium-90 transarterial radioembolization (TARE) in patients with hepatocellular carcinoma (HCC), using a quantitative assessment of dynamic computed tomography (CT) images.
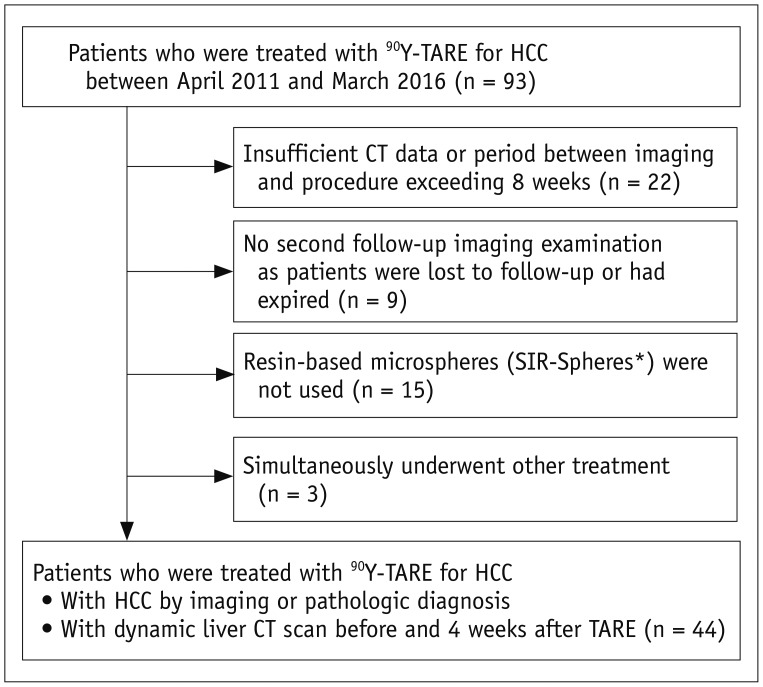
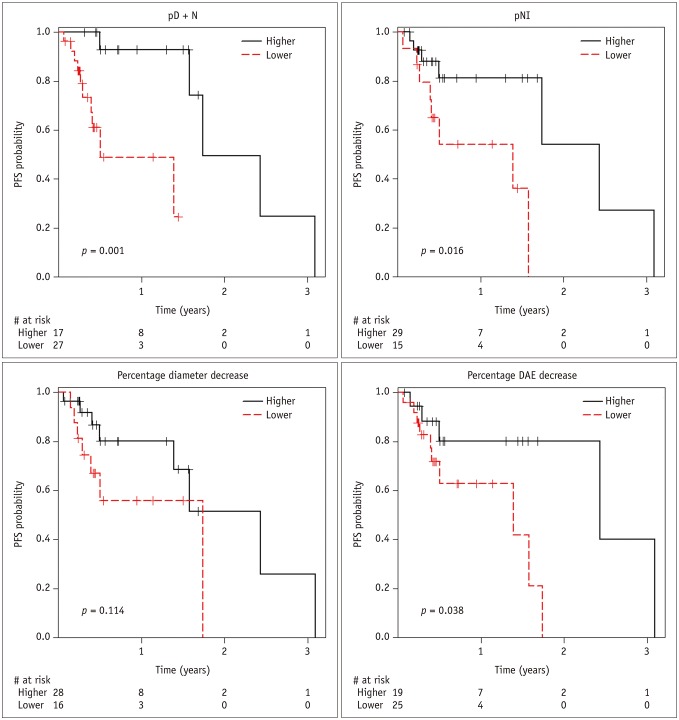
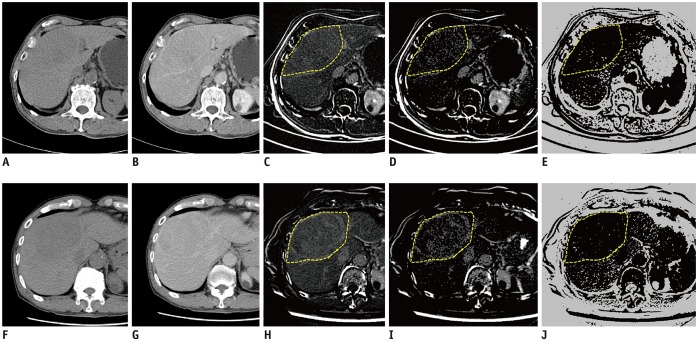
Dynamic contrast-enhanced CT was obtained pre- and 4 weeks post-TARE in 44 patients (34 men, 10 women; mean age, 60 years) with HCC. Computer software was developed for measuring the percentage increase in the combined delayed-enhancing area and necrotic area (pD + N) and the percentage increase in the necrotic area (pNI) in the tumor-containing segments pre- and post-TARE. Local progression-free survival (PFS) was compared between patient groups using Cox regression and Kaplan-Meier analyses.
Post-TARE HCC with pD + N ≥ 35.5% showed significantly longer PFS than those with pD + N < 35.5% ( = 0.001). The local tumor progression hazard ratio was 17.3 ( = 0.009) for pD + N < 35.5% versus pD + N ≥ 35.5% groups. HCCs with a high pNI tended to have longer PFS, although this difference did not reach statistical significance.
HCCs with a larger pD + N are less likely to develop local progression after TARE.
利用动态计算机断层扫描(CT)图像的定量评估,确定用于评估钇 90 经动脉放射栓塞(TARE)治疗肝细胞癌(HCC)早期治疗反应的影像学预测因子。
对 44 例 HCC 患者(34 名男性,10 名女性;平均年龄 60 岁)在 TARE 前和 TARE 后 4 周进行了动态对比增强 CT 检查。开发了计算机软件来测量 TARE 前后肿瘤所在节段的联合延迟强化面积和坏死面积(pD + N)的百分比增加以及坏死面积(pNI)的百分比增加。使用 Cox 回归和 Kaplan-Meier 分析比较了不同患者组之间的局部无进展生存期(PFS)。
pD + N ≥ 35.5%的 TARE 后 HCC 患者的 PFS 明显长于 pD + N < 35.5%的患者( = 0.001)。pD + N < 35.5%与 pD + N ≥ 35.5%组相比,局部肿瘤进展的危险比为 17.3( = 0.009)。pNI 较高的 HCC 患者 PFS 较长,但差异无统计学意义。
pD + N 较大的 HCC 患者在 TARE 后发生局部进展的可能性较小。