Department of Internal Medicine, Respirology and Critical Illness Division, Faculty of Medicine Universitas Padjadjaran, Hasan Sadikin General Hospital, Bandung, Indonesia.
Department of Public Health, Faculty of Medicine Universitas Padjadjaran, Bandung, Indonesia.
PLoS One. 2019 Feb 28;14(2):e0213017. doi: 10.1371/journal.pone.0213017. eCollection 2019.
Rifampicin-resistant tuberculosis (RR-TB) is largely underdetected in Indonesia. Xpert MTB/RIF (Xpert) has recently been introduced, prioritizing patients at risk of RR-TB, followed by phenotypic drug-susceptibility (DST) if rifampicin resistance is detected.
This study investigated Xpert-based management of presumptive RR-TB cases under routine practice in West Java, Indonesia.
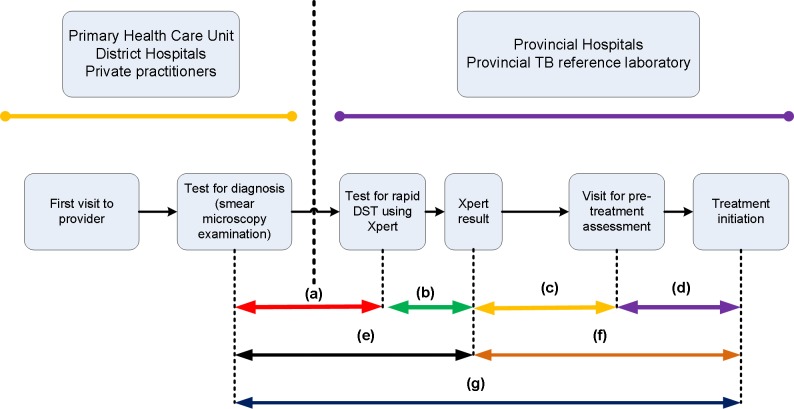
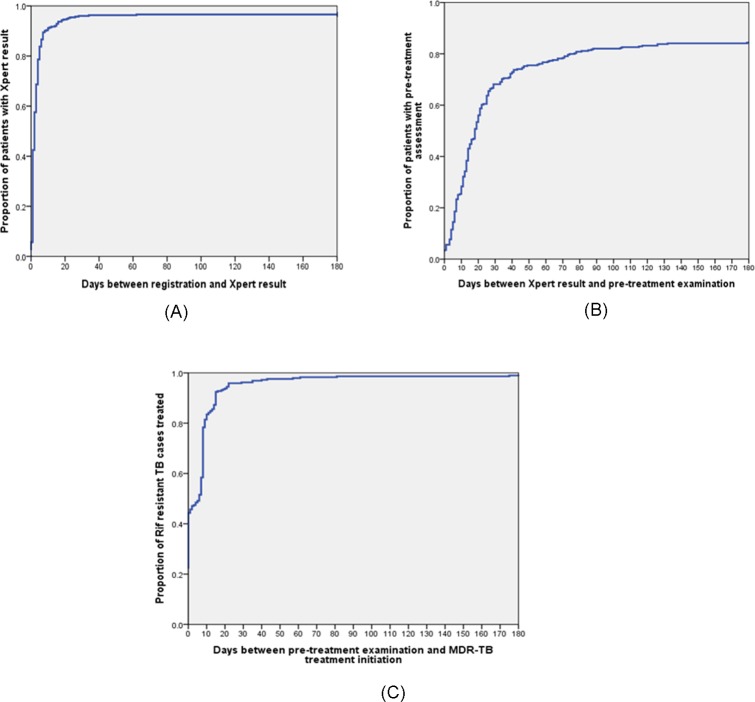
We examined all records of patients tested with Xpert in the referral hospital for West Java in 2015-2016. We measured loss across a limited cascade of care, time to Xpert diagnosis and the commencement of initial second-line treatment, and identified factors associated with diagnostic and treatment delay. Additionally, we analyzed the appropriateness of treatment according to DST results.
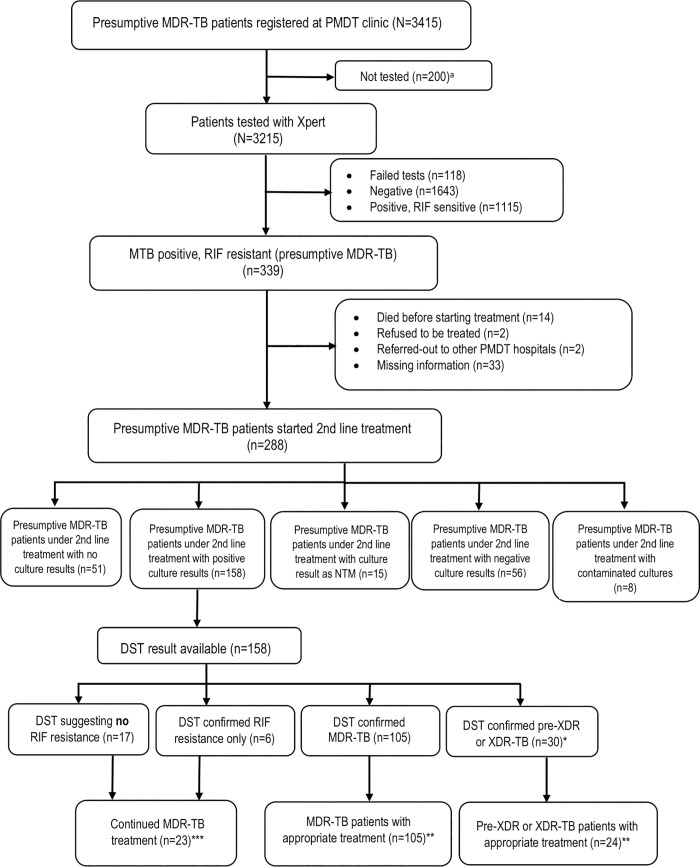
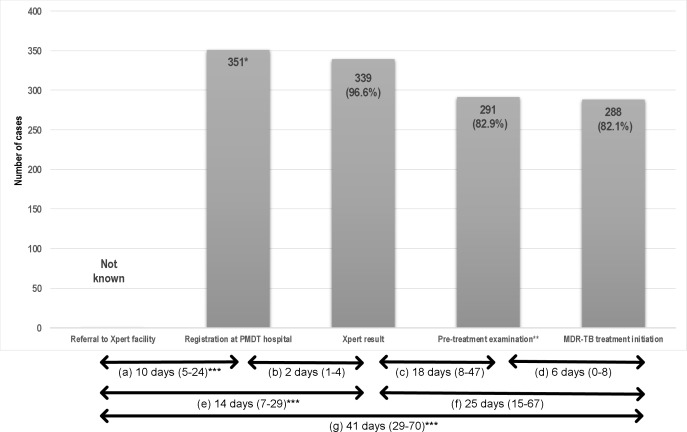
Of 3415 patients with presumptive RR-TB, 3215 (94%) were tested by Xpert, of whom 339 (10.5%) were diagnosed as RR-TB. 288 (85%) of 339 RR-TB patients started initial second-line TB treatment, with 48 (14%) patients being lost between diagnosis and pre-treatment assessment. Second-line treatment was commenced at a median of 41 days (IQR 29-70) after RR-TB diagnosis. Delays in both diagnosis and treatment initiation were observed in 104 (52%) of 201 RR-TB patients with identifiable referral date. Rural residence was associated with delay to diagnosis (adjusted OR 2.7; 95%CI 1.5-5.2) and treatment initiation (adjusted OR 2.0; 1.2-3.4). Of 162 patients with available DST result, 107 (66%) had multidrug-resistant tuberculosis (MDR-TB) and 32 (20%) had either pre-extensively drug resistant (pre-XDR) or extensively drug resistant tuberculosis (XDR-TB). We estimated that with the current algorithm 41% of pre-XDR or XDR-TB patients are diagnosed, and 33% of them started on an appropriate treatment regimen.
Many patients with Xpert-diagnosed RR-TB either do not start MDR-TB treatment or encountered diagnostic and treatment delays under programmatic conditions in Indonesia, and most pre-XDR and XDR-TB cases remain undiagnosed. Further expansion and ongoing quality improvement of RR-TB services are urgently needed.
在印度尼西亚,利福平耐药结核病(RR-TB)的检出率普遍较低。最近引入了 Xpert MTB/RIF(Xpert),优先考虑 RR-TB 风险患者,如果检出利福平耐药,则进行表型药物敏感性(DST)检测。
本研究调查了在印度尼西亚西爪哇常规实践中基于 Xpert 的疑似 RR-TB 病例的管理。
我们检查了 2015-2016 年在西爪哇转诊医院接受 Xpert 检测的所有患者的记录。我们测量了有限的护理级联中的损失、Xpert 诊断时间和开始初始二线治疗的时间,并确定了与诊断和治疗延迟相关的因素。此外,我们根据 DST 结果分析了治疗的适当性。
在 3415 例疑似 RR-TB 患者中,有 3215 例(94%)接受了 Xpert 检测,其中 339 例(10.5%)被诊断为 RR-TB。339 例 RR-TB 患者中有 288 例(85%)开始接受初始二线结核病治疗,其中 48 例(14%)患者在诊断和治疗前评估之间失访。二线治疗在 RR-TB 诊断后中位数 41 天(IQR 29-70)开始。在可确定转诊日期的 201 例 RR-TB 患者中,有 104 例(52%)观察到诊断和治疗开始延迟。农村居住与诊断延迟(调整比值比 2.7;95%CI 1.5-5.2)和治疗开始延迟(调整比值比 2.0;1.2-3.4)相关。在 162 例可获得 DST 结果的患者中,107 例(66%)患有耐多药结核病(MDR-TB),32 例(20%)患有预广泛耐药(pre-XDR)或广泛耐药结核病(XDR-TB)。我们估计,根据当前的算法,41%的预 XDR 或 XDR-TB 患者得到诊断,其中 33%的患者开始接受适当的治疗方案。
在印度尼西亚的规划方案中,许多 Xpert 诊断的 RR-TB 患者要么没有开始 MDR-TB 治疗,要么出现诊断和治疗延迟,而且大多数预 XDR 和 XDR-TB 病例仍未得到诊断。迫切需要进一步扩大和持续改进 RR-TB 服务。