Division of Medical Microbiology, University of Cape Town, Cape Town, South Africa, Division of Tuberculosis Elimination, Centers for Disease Control and Prevention, Atlanta, Georgia, USA.
Centre for Infectious Disease Research, University of Cape Town, Cape Town, South Africa.
Int J Tuberc Lung Dis. 2017 Nov 1;21(11):1173-1180. doi: 10.5588/ijtld.17.0230.
To reduce transmission and improve patient outcomes, rapid diagnosis and treatment of rifampicin-resistant tuberculosis (RR-TB) is required.
To conduct a systematic review and meta-analysis assessing time to treatment for RR-TB and variability using diagnostic testing methods and treatment delivery approach.
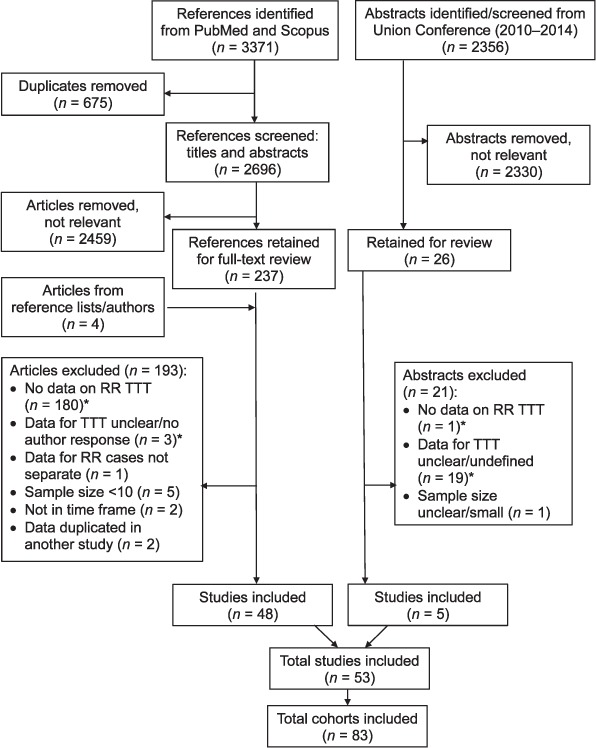
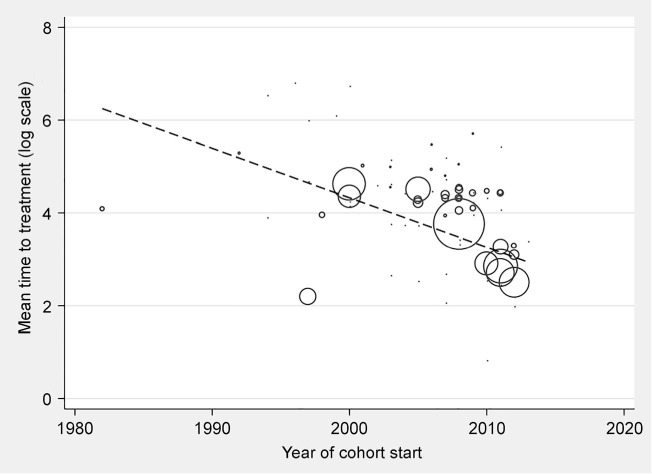
Studies from 2000 to 2015 reporting time to second-line treatment initiation were selected from PubMed and published conference abstracts.
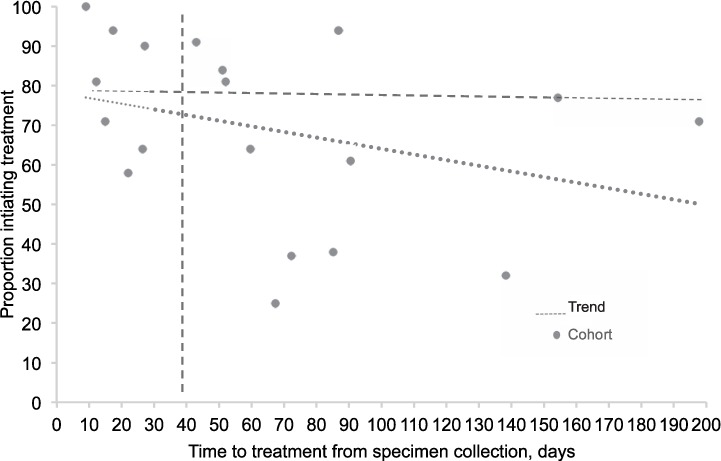
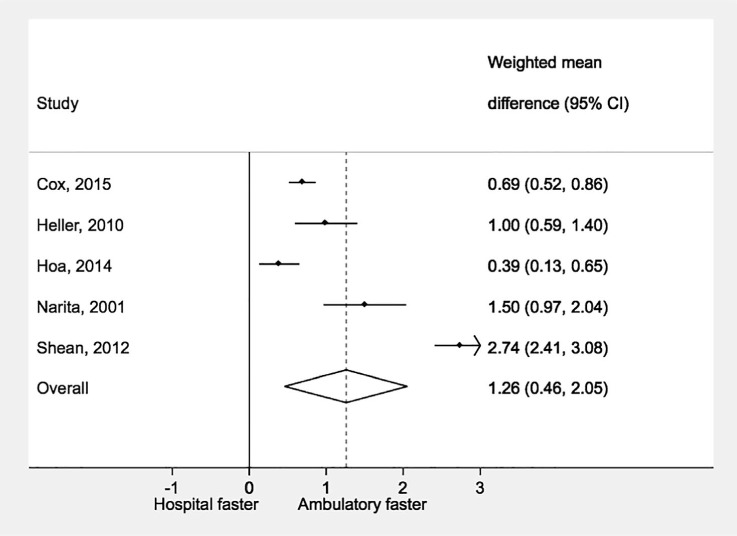
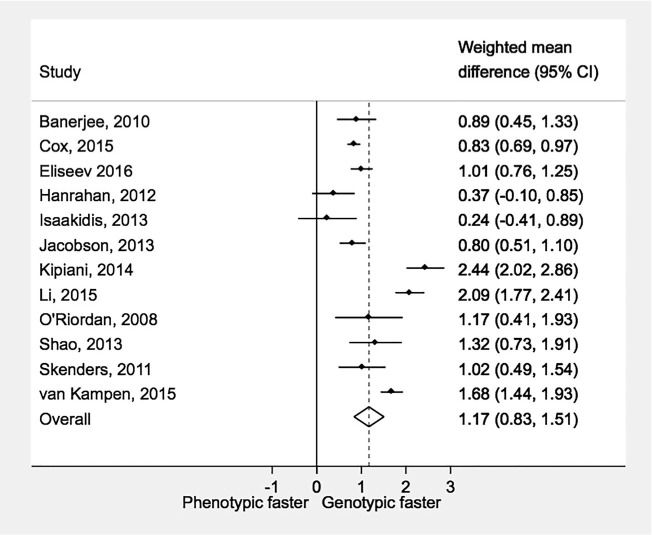
From 53 studies, 83 cohorts (13 034 patients) were included. Overall weighted mean time to treatment from specimen collection was 81 days (95%CI 70-91), and was shorter with ambulatory (57 days, 95%CI 40-74) than hospital-based treatment (86 days, 95%CI 71-102). Time to treatment was shorter with genotypic susceptibility testing (38 days, 95%CI 27-49) than phenotypic testing (108 days, 95%CI 98-117). The mean percentage of diagnosed patients initiating treatment was 76% (95%CI 70-83, range 25-100).
Time to second-line anti-tuberculosis treatment initiation is extremely variable across studies, and often unnecessarily long. Reduced delays are associated with genotypic testing and ambulatory treatment settings. Routine monitoring of the proportion of diagnosed patients initiating treatment and time to treatment are necessary to identify areas for intervention.
为了减少传播并改善患者的预后,需要快速诊断和治疗利福平耐药结核病(RR-TB)。
对使用诊断检测方法和治疗提供方法评估 RR-TB 治疗时间和变异性的系统评价和荟萃分析。
从 2000 年到 2015 年,从 PubMed 和已发表的会议摘要中选择了报告二线治疗开始时间的研究。
从 53 项研究中,纳入了 83 个队列(13034 名患者)。从标本采集到治疗的总体加权平均治疗时间为 81 天(95%CI 70-91),与基于门诊的治疗(57 天,95%CI 40-74)相比,住院治疗(86 天,95%CI 71-102)较短。与表型检测(108 天,95%CI 98-117)相比,基因型药敏检测(38 天,95%CI 27-49)的治疗时间更短。开始治疗的确诊患者的平均比例为 76%(95%CI 70-83,范围 25-100)。
二线抗结核治疗开始时间在不同研究之间差异极大,而且往往不必要地延长。减少延迟与基因型检测和门诊治疗环境有关。常规监测开始治疗的确诊患者比例和治疗时间对于确定干预领域是必要的。