Department of Cardiology, the fourth Affiliated Hospital of China Medical University, Shenyang, 110032, Liaoning, China.
BMC Cardiovasc Disord. 2019 Mar 1;19(1):49. doi: 10.1186/s12872-019-1022-6.
Approximately 30-50% patients with acute ST-segment elevation myocardial infarction (STMEI) were found to have non-infarct-related coronary artery (IRA) disease, which was significantly associated with worse prognosis. However, challenges still remain for these patients: which non-infarct-related lesion should be treated and when should the procedure be performed? The present study aims to investigate Fractional flow reserve (FFR)-guided complete revascularization (CR) in comparison to culprit-only revascularization (COR) in patients with ST-segment elevation myocardial infarction (STEMI) and multi-vessel disease (MVD).
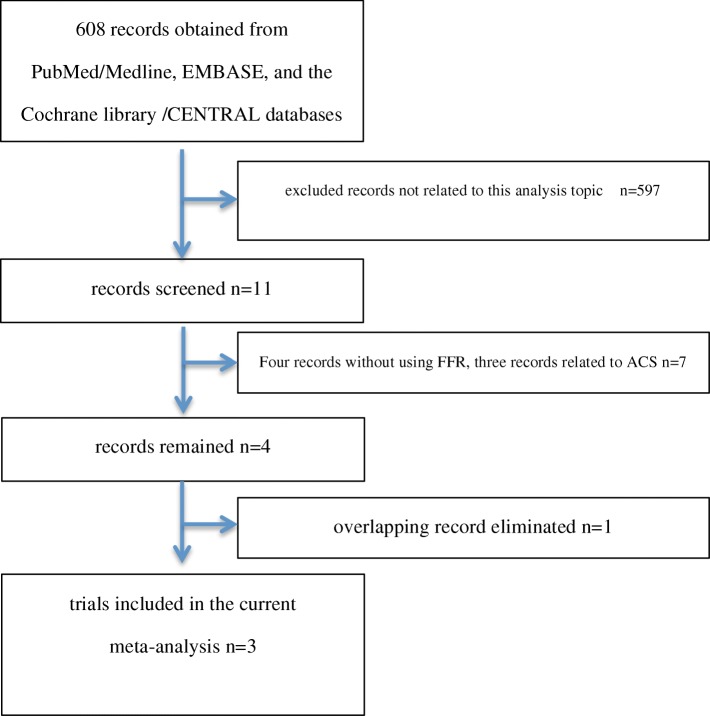
Three appropriate randomized controlled trials (RCTs) were selected from the PubMed/Medline, EMBASE, and the Cochrane library /CENTRAL databases. 1631 patients (688 patients underwent FFR-guided CR and 943 patients underwent COR) following-up 12-44 months was evaluated.
FFR-guided CR significantly reduced major adverse cardiac event (MACE) (OR 0.47, 95% CI: 0.35-0.62, P < 0.00001) and ischemia-driven repeat revascularization (OR 0.36, 0.26-0.51, P < 0.00001), as compared to COR. However, there is no difference in all-cause mortality (OR 1.24, 0.65-2.35, P = 0.51).
In patients with STEMI and MVD, FFR-guided CR is better than COR in terms of MACE and ischemia-driven repeat revascularization, while there are almost similar in all-cause mortality.
All analyses were based on previous published studies, thus no ethical approval and patient consent are required COMPARE-ACUTE trial number NCT01399736 ; DANAMI-3-PRIMULTI trial number NCT01960933 .
约 30-50%急性 ST 段抬高型心肌梗死(STEMI)患者存在非梗死相关动脉(IRA)病变,其与更差的预后显著相关。然而,这些患者仍然存在挑战:应治疗哪支非梗死相关病变,以及何时进行介入治疗?本研究旨在探讨血流储备分数(FFR)指导的完全血运重建(CR)与罪犯血管血运重建(COR)在 STEMI 合并多支血管病变(MVD)患者中的疗效比较。
从 PubMed/Medline、EMBASE 和 Cochrane 图书馆/CENTRAL 数据库中筛选出三项合适的随机对照试验(RCT)。共纳入 1631 例患者(688 例行 FFR 指导的 CR,943 例行 COR),随访 12-44 个月。
与 COR 相比,FFR 指导的 CR 可显著降低主要不良心脏事件(MACE)(OR 0.47,95%CI:0.35-0.62,P<0.00001)和缺血驱动的再次血运重建(OR 0.36,0.26-0.51,P<0.00001),但两组全因死亡率无差异(OR 1.24,0.65-2.35,P=0.51)。
对于 STEMI 合并 MVD 患者,与 COR 相比,FFR 指导的 CR 可降低 MACE 和缺血驱动的再次血运重建发生率,但全因死亡率无差异。
所有分析均基于已发表的研究,因此无需伦理批准和患者同意 COMPARE-ACUTE 试验注册号:NCT01399736;DANAMI-3-PRIMULTI 试验注册号:NCT01960933。