Department of Laboratory Medicine, University of Debrecen, Nagyerdei krt. 98, Debrecen, H-4032, Hungary.
Department of Internal Medicine, Faculty of Medicine, University of Debrecen, Debrecen, Hungary.
Ann Hematol. 2019 Jun;98(6):1413-1420. doi: 10.1007/s00277-019-03642-w. Epub 2019 Mar 4.
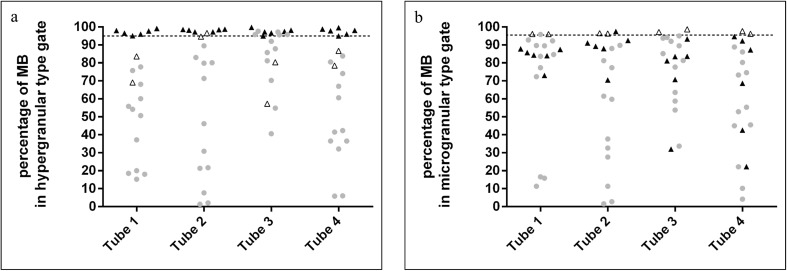
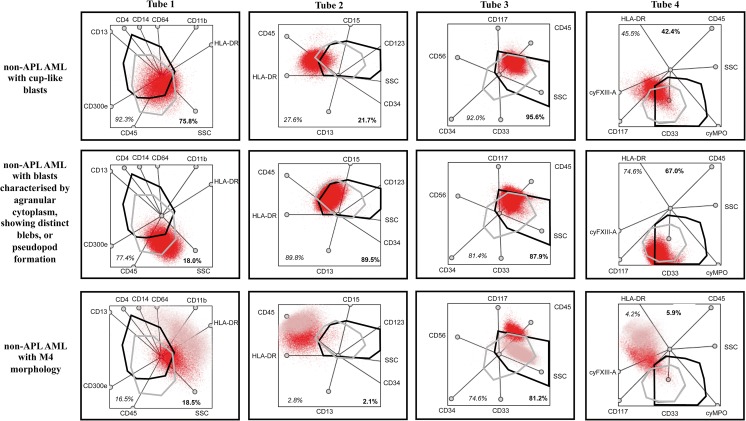
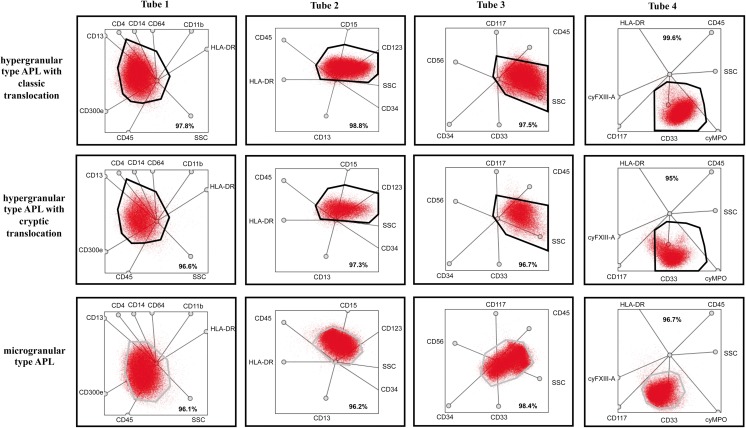
Acute promyelocytic leukemia (APL) is generally characterized by t(15;17)(q24;q21). In some cases, the classic translocation cannot be identified by conventional methods, since the PML-RARA fusion protein results from complex, variant, or cryptic translocation. The diagnostic algorithm of APL starts with screening methods, such as flow cytometry (FC), followed by fluorescence in situ hybridization or polymerase chain reaction to confirm the diagnosis. Our aim was to develop a novel protocol for analyzing APL samples based on multidimensional dot-plots that can provide comprehensive information about several markers at the same time. The protocol included four optimized multidimensional dot-plots, which were tested by retrospective reanalysis of FC results in APL (n = 8) and non-APL (n = 12) acute myeloid leukemia (AML) cases. After predicting the potential position of hypergranular- and microgranular-type aberrant promyelocytes, the percentages of blast populations were examined within the gates in all AML cases. The percentage of blasts in each predefined gate was well above the cut-off value (95%) in APL cases in all tubes. In non-APL AML cases, the percentage of blasts in the same gates never reached the cut-off value in all investigated tubes, and even when it did in a single tube, the pattern was markedly different from that observed in APL cases. In conclusion, multidimensional dot-plots can be used for screening APL even in cryptic APL cases, although reproducibility across several laboratories would require standardization of antibodies and fluorochromes. This easy-to-use and quick method can support the diagnosis of APL and the prompt initiation of the appropriate treatment.
急性早幼粒细胞白血病(APL)通常表现为 t(15;17)(q24;q21)。在某些情况下,由于 PML-RARA 融合蛋白源自复杂、变体或隐匿性易位,常规方法无法识别经典易位。APL 的诊断算法始于筛选方法,如流式细胞术(FC),然后通过荧光原位杂交或聚合酶链反应来确认诊断。我们的目的是开发一种新的基于多维点图的 APL 样本分析方案,该方案可以同时提供多个标记物的综合信息。该方案包括四个优化的多维点图,通过对 APL(n=8)和非 APL(n=12)急性髓系白血病(AML)病例的 FC 结果进行回顾性重新分析来测试该方案。在预测了超颗粒型和微颗粒型异常早幼粒细胞的潜在位置后,在所有 AML 病例中检查了门内的原始细胞群体百分比。在所有试管中,APL 病例中每个预定义门内的原始细胞百分比均远高于截止值(95%)。在非 APL AML 病例中,同一门内的原始细胞百分比在所有研究的试管中从未达到截止值,即使在单个试管中达到,其模式也与 APL 病例明显不同。总之,多维点图可用于筛选 APL,即使是隐匿性 APL 病例,尽管需要标准化抗体和荧光染料才能在多个实验室中具有可重复性。这种易于使用且快速的方法可以支持 APL 的诊断,并及时开始适当的治疗。