Department of VIP, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, 600 Yishan Road, Shanghai, 200233, China.
Department of Cardiology, Shanghai Jiao Tong University Affiliated Sixth People's Hospital, 600 Yishan Road, Shanghai, 200233, China.
BMC Cardiovasc Disord. 2019 Mar 4;19(1):50. doi: 10.1186/s12872-019-1027-1.
Both nonthyroidal illness syndrome and renal dysfunction are associated with increased mortality risk in acute myocardial infarction (AMI). However, it is unclear whether combined NTIS and renal dysfunction further increase mortality risk. Therefore, our aim is to investigate whether combined NTIS and renal dysfunction further increases mortality risk in patients with acute myocardial infarction (AMI).
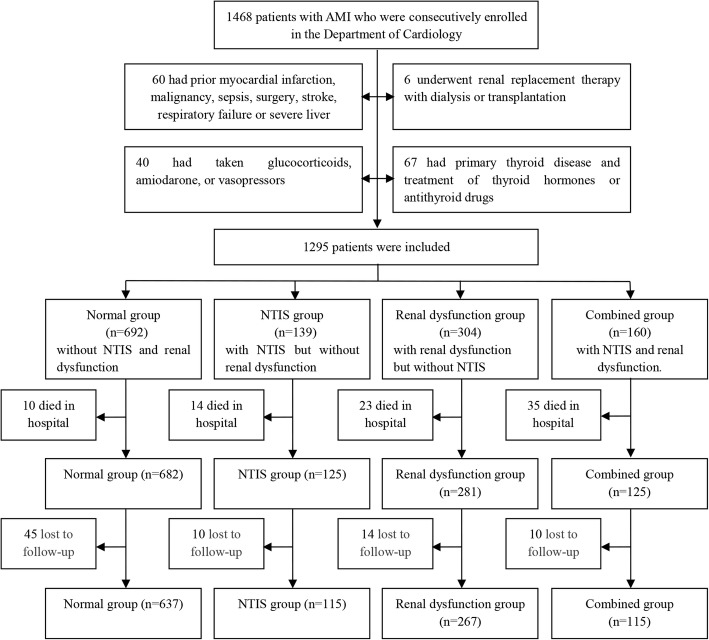
A total of 1295 inpatients with AMI were divided into normal group (n = 692), NTIS group (n = 139), renal dysfunction group (n = 304), and combined NTIS and renal dysfunction group (n = 160). Heart function, in-hospital, all-cause and cardiovascular mortality were compared among the four groups.
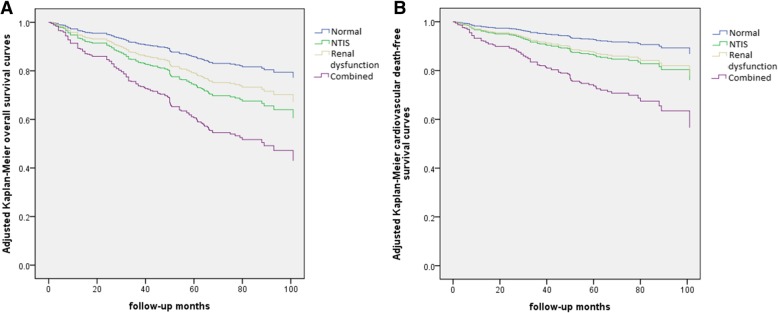
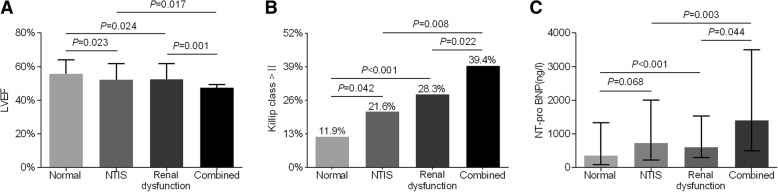
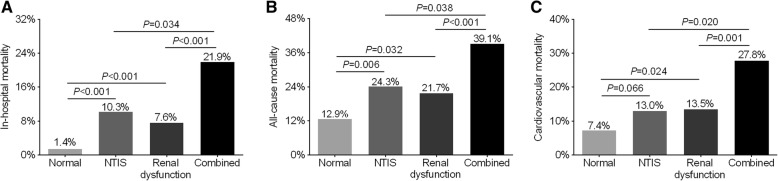
After adjustment for age and sex, left ventricular ejection fraction was significantly lower in the combined group (48 ± 11%) than in the NTIS group (52 ± 10%, P = 0.017), the renal dysfunction group (52 ± 10%, P = 0.001) and the normal group (56 ± 8%, P < 0.001). After controlling for confounding factors, compared with the normal group, the NTIS and the renal dysfunction group represented higher risks of in-hospital mortality (OR: 3.643, P = 0.028; OR:3.135, P = 0.042, respectively), all-cause mortality (HR: 2.138, P = 0.007; HR: 2.050, P = 0.003, respectively), and cardiovascular mortality (HR:2.134, P = 0.042; HR:2.237, P = 0.010, respectively). Compared to those in the NTIS and the renal dysfunction group, the patients in the combined group showed a further increased risk for in-hospital mortality (OR:2.916, P = 0.039; OR:2.487, P = 0.036, respectively), all-cause mortality (HR: 1.939, P = 0.015; HR: 2.020, P = 0.002, respectively) and cardiovascular mortality (HR:2.420, P = 0.010; HR:2.303, P = 0.002, respectively).
Both NTIS and renal dysfunction increase short-term in-hospital mortality, and long-term all-cause and cardiovascular mortality risk in patients with AMI. Furthermore, the coexistence of NTIS and renal dysfunction presents further increased mortality risk in AMI patients.
非甲状腺病态综合征和肾功能障碍与急性心肌梗死(AMI)患者的死亡风险增加有关。然而,尚不清楚联合 NTIS 和肾功能障碍是否会进一步增加死亡风险。因此,我们的目的是研究联合 NTIS 和肾功能障碍是否会进一步增加急性心肌梗死(AMI)患者的死亡风险。
共纳入 1295 例 AMI 住院患者,分为正常组(n=692)、NTIS 组(n=139)、肾功能障碍组(n=304)和联合 NTIS 和肾功能障碍组(n=160)。比较四组患者的心功能、住院期间、全因和心血管死亡率。
校正年龄和性别后,联合组左心室射血分数(48±11%)明显低于 NTIS 组(52±10%,P=0.017)、肾功能障碍组(52±10%,P=0.001)和正常组(56±8%,P<0.001)。在控制混杂因素后,与正常组相比,NTIS 组和肾功能障碍组住院期间死亡率(OR:3.643,P=0.028;OR:3.135,P=0.042)、全因死亡率(HR:2.138,P=0.007;HR:2.050,P=0.003)和心血管死亡率(HR:2.134,P=0.042;HR:2.237,P=0.010)风险均升高。与 NTIS 组和肾功能障碍组相比,联合组住院期间死亡率(OR:2.916,P=0.039;OR:2.487,P=0.036)、全因死亡率(HR:1.939,P=0.015;HR:2.020,P=0.002)和心血管死亡率(HR:2.420,P=0.010;HR:2.303,P=0.002)风险进一步升高。
NTIS 和肾功能障碍均增加 AMI 患者短期住院期间死亡率和长期全因及心血管死亡率风险。此外,NTIS 和肾功能障碍并存会进一步增加 AMI 患者的死亡风险。