School of Pharmacy, Royal College of Surgeons in Ireland, Dublin, Ireland.
Department of General Practice, HRB Centre for Primary Care Research, Royal College of Surgeons in Ireland, Dublin, Ireland.
BMJ Open. 2019 Mar 4;9(3):e022927. doi: 10.1136/bmjopen-2018-022927.
Growing evidence suggests that older adults are at an increased risk of injurious falls when initiating antihypertensive medication, while the evidence regarding long-term use of antihypertensive medication and the risk of falling is mixed. However, long-term users who stop and start these medications may have a similar risk of falling to initial users of antihypertensive medication. Our aim was to evaluate the association between gaps in antihypertensive medication adherence and injurious falls in older (≥65 years) community-dwelling, long-term (≥≥1 year) antihypertensive users.
Prospective cohort study.
Irish Community Pharmacy.
Consecutive participants presenting a prescription for antihypertensive medication to 106 community pharmacies nationwide, community-dwelling, ≥65 years, with no evidence of cognitive impairment, taking antihypertensive medication for ≥1 year (n=938).
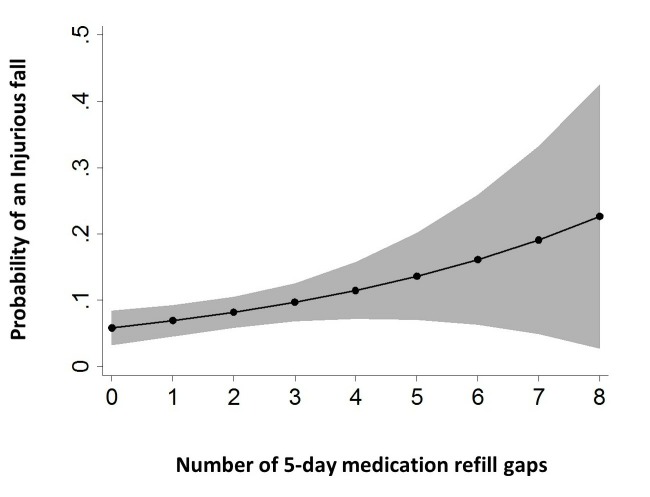
Gaps in antihypertensive medication adherence were evaluated from linked dispensing records as the number of 5-day gaps between sequential supplies over the 12-month period prior to baseline. Injurious falls during follow-up were recorded via questionnaire during structured telephone interviews at 12 months.
At 12 months, 8.1% (n=76) of participants reported an injurious fall requiring medical attention. The mean number of 5-day gaps in medication refill behaviour was 1.47 . In adjusted, modified Poisson models, 5-day medication refill gaps at baseline were associated with a higher risk of an injurious fall during follow-up (aRR 1.18, 95% CI 1.02 to 1.37, =0.024).
Each 5-day gap in antihypertensive refill adherence increased the risk of self-reported injurious falls by 18%. Gaps in antihypertensive adherence may be a marker for increased risk of injurious falls. It is unknown whether adherence-interventions will reduce subsequent risk. This finding is hypothesis generating and should be replicated in similar populations.
越来越多的证据表明,老年人在开始使用降压药物时受伤性跌倒的风险增加,而关于长期使用降压药物与跌倒风险的证据则存在差异。然而,停止和开始使用这些药物的长期使用者跌倒的风险可能与初始使用降压药物的使用者相似。我们的目的是评估降压药物依从性中断与老年(≥65 岁)社区居住、长期(≥≥1 年)使用降压药物的患者受伤性跌倒之间的关联。
前瞻性队列研究。
爱尔兰社区药房。
向全国 106 家社区药房连续呈现降压药物处方的参与者,社区居住,年龄≥65 岁,无认知障碍证据,服用降压药物≥1 年(n=938)。
通过链接配药记录评估降压药物依从性中断情况,即在基线前 12 个月内,连续供应之间出现 5 天的药物供应中断次数。在 12 个月的随访期间,通过结构电话访谈记录受伤性跌倒情况。
在 12 个月时,8.1%(n=76)的参与者报告了需要医疗关注的受伤性跌倒。药物补充行为中 5 天药物供应中断的平均次数为 1.47。在调整后的修正泊松模型中,基线时 5 天的药物补充中断与随访期间受伤性跌倒的风险增加相关(调整后的相对风险 1.18,95%置信区间 1.02 至 1.37,=0.024)。
降压药物补充依从性每出现 5 天的中断,自我报告的受伤性跌倒风险就会增加 18%。降压药物依从性中断可能是受伤性跌倒风险增加的标志。尚不清楚依从性干预是否会降低随后的风险。这一发现是假设性的,应该在类似人群中进行复制。