Nepean Hospital, Sydney, NSW, Australia.
Medical ICU, Amiens University Hospital, Amiens, France.
Crit Care. 2019 Mar 7;23(1):70. doi: 10.1186/s13054-019-2375-z.
Right ventricle (RV) size and function assessment by echocardiography (echo) is a standard tool in the ICU. Frequently subjective assessment is performed, and guidelines suggest its utility in adequately trained clinicians. We aimed to compare subjective (visual) assessment of RV size and function by ICU physicians, with advanced qualifications in echocardiography, vs objective measurements.
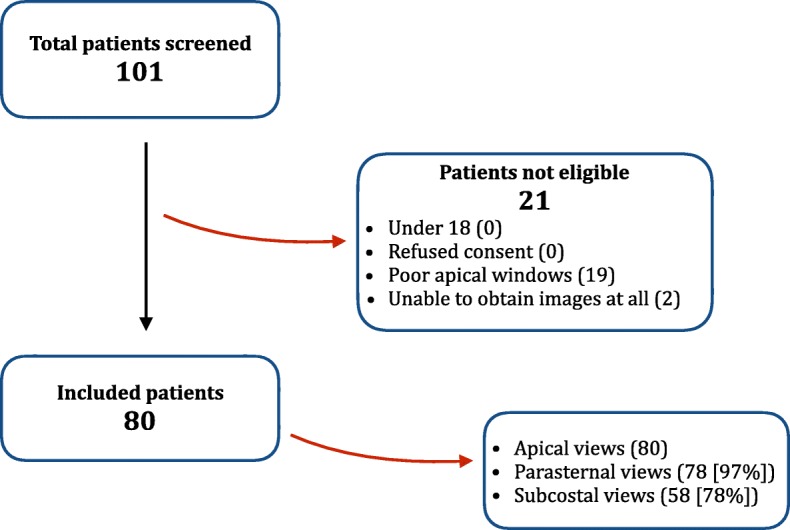
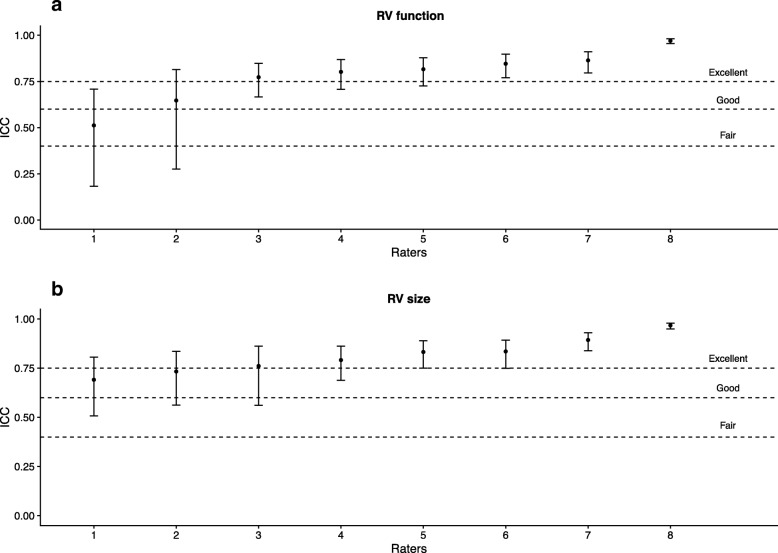
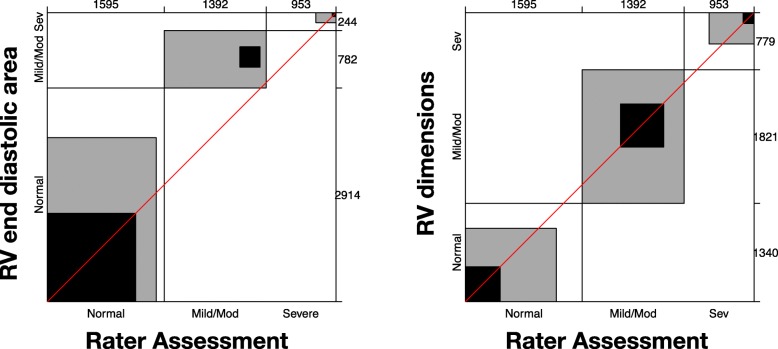
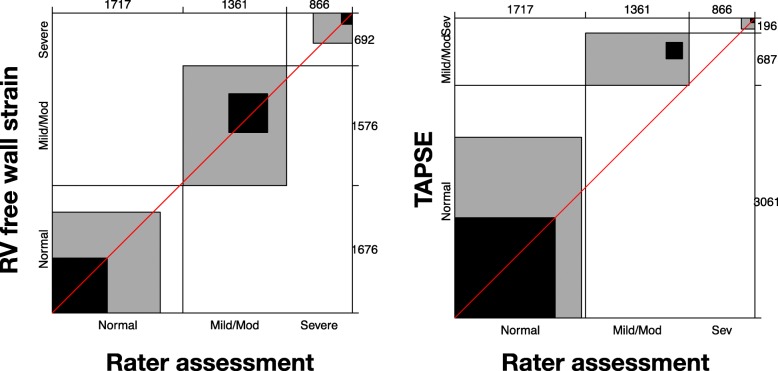
ICU specialists with a qualification in advanced echocardiography reviewed 2D echo clips from critically ill patients on mechanical ventilation with PaO:FiO < 300. Subjective assessments of RV size and function were made independently using a three-class categorical scale. Agreement (B-score) and bias (p value) were analysed using objective echo measurements. RV size assessment included RV end-diastolic area (EDA) and diameters. RV function assessment included fractional area change, S', TAPSE and RV free wall strain. Binary and ordinal analysis was performed.
Fifty-two clinicians reviewed 2D images from 80 patients. Fair agreement was seen with objective measures vs binary assessment of RV size (RV EDA 0.26 [p < 0.001], RV dimensions 0.29 [p = 0.06]) and function (RV free wall strain 0.27 [p < 0.001], TAPSE 0.27 [p < 0.001], S' 0.29 [p < 0.001], FAC 0.31 [p = 0.16]). However, ordinal data analysis showed poor agreement with RV dimensions (0.11 [p = 0.06]) and RV free wall strain (0.14 [p = 0.16]). If one-step disagreement was allowed, agreement was good (RV dimensions 0.6 [p = 0.06], RV free wall strain 0.6 [p = 0.16]). Significant overestimation of severity of abnormalities was seen with subjective assessment vs RV EDA, TAPSE, S' and fractional area change.
Subjective (visual) assessment of RV size and function, by ICU specialists trained in advanced echo, can be fairly reliable for the initial exclusion of significant RV pathology. It seems prudent to avoid subjective RV assessment in isolation.
超声心动图(echo)评估右心室(RV)大小和功能是 ICU 的标准工具。通常进行主观评估,指南建议在经过充分培训的临床医生中使用该方法。我们旨在比较 ICU 医生的 RV 大小和功能的主观(视觉)评估与客观测量值。
具有高级超声心动图资格的 ICU 专家对接受机械通气且 PaO:FiO<300 的重症患者的 2D 超声心动图片段进行了回顾。使用三分类类别量表独立进行 RV 大小和功能的主观评估。使用客观的超声心动图测量值分析了一致性(B 评分)和偏差(p 值)。RV 大小评估包括 RV 舒张末期面积(EDA)和直径。RV 功能评估包括射血分数、S'、TAPSE 和 RV 游离壁应变。进行了二项式和有序分析。
52 名临床医生对 80 名患者的 2D 图像进行了评估。与 RV 大小的客观测量值相比,与 RV EDA(0.26,p<0.001)和 RV 尺寸(0.29,p=0.06)的二进制评估具有公平的一致性,与 RV 功能(RV 游离壁应变 0.27,p<0.001)、TAPSE 0.27(p<0.001)、S'0.29(p<0.001)和 FAC 0.31(p=0.16)的一致性也较好。然而,有序数据分析显示与 RV 尺寸(0.11,p=0.06)和 RV 游离壁应变(0.14,p=0.16)的一致性较差。如果允许一步不一致,一致性则较好(RV 尺寸 0.6,p=0.06;RV 游离壁应变 0.6,p=0.16)。与 RV EDA、TAPSE、S'和射血分数相比,主观评估会明显高估 RV 异常的严重程度。
受过高级超声心动图培训的 ICU 专家的 RV 大小和功能的主观(视觉)评估可以较为可靠地初步排除 RV 病变。似乎明智的做法是避免单独进行主观 RV 评估。