Center for Pulmonary Imaging Research, Division of Pulmonary Medicine and Dept of Radiology, Cincinnati Children's Hospital Medical Center, Cincinnati, OH, USA.
Dept of Pediatrics, College of Medicine, University of Cincinnati, Cincinnati, OH, USA.
Eur Respir J. 2019 May 2;53(5). doi: 10.1183/13993003.01779-2018. Print 2019 May.
Early detection of pulmonary morbidity following haematopoietic stem cell transplantation (HSCT) remains an important challenge for intervention, primarily due to the insensitivity of spirometry to early change, and in paediatrics, patient compliance provides additional challenges. Regional lung ventilation abnormalities in paediatric HSCT patients were quantified using hyperpolarised xenon-129 (Xe) magnetic resonance imaging (MRI) and compared to spirometry.
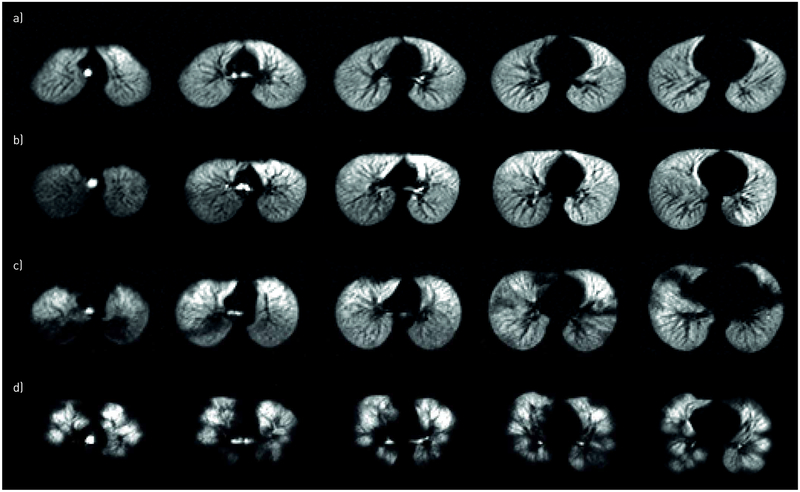
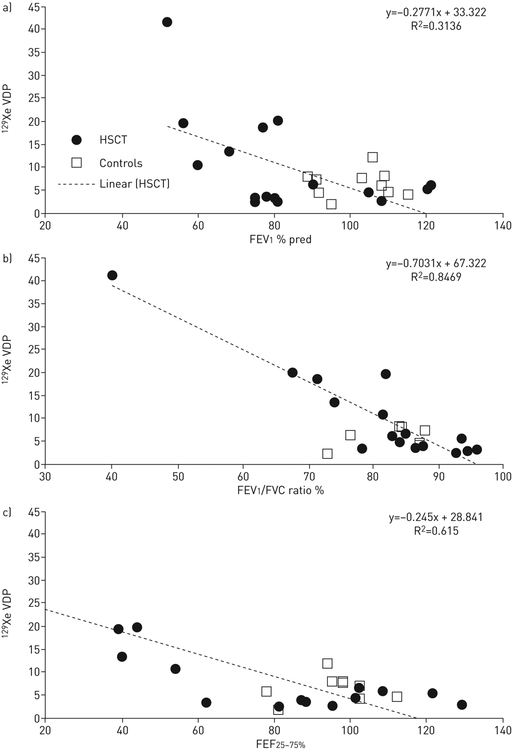
Medically stable, paediatric allogeneic HSCT patients (n=23, ages 6-16 years) underwent an outpatient MRI scan where regional ventilation was quantified with a breath-hold of hyperpolarised Xe gas. Ventilation deficits, regions of the lung that ventilate poorly due to obstruction, were quantified as a ventilation defect percentage (VDP) and compared to forced expiratory volume in 1 s (FEV), FEV/forced vital capacity (FVC) ratio, and forced expiratory flow at 25-75% of FVC (FEF) from spirometry using linear regression.
The mean±sd Xe VDP was 10.5±9.4% (range 2.6-41.4%). Xe VDP correlated with FEV, FEV/FVC ratio and FEF (p≤0.02 for all comparisons). Ventilation deficits were detected in patients with normal spirometry ( FEV >80%), supporting the sensitivity of Xe MRI to early obstruction reported in other pulmonary conditions. Seven (30%) patients could not perform spirometry, yet ventilation deficits were observed in five of these patients, detecting abnormalities that otherwise may have gone undetected and untreated until advanced.
Lung ventilation deficits were detected using hyperpolarised Xe gas MRI in asymptomatic paediatric HSCT patients and in a subgroup who were unable to perform reliable spirometry. Xe MRI provides a reliable imaging-based assessment of pulmonary involvement in this potentially difficult to diagnose paediatric population.
造血干细胞移植(HSCT)后肺部发病率的早期检测仍然是干预的一个重要挑战,主要是因为肺活量测定法对早期变化不敏感,而在儿科中,患者的依从性带来了额外的挑战。本研究使用超极化氙-129(Xe)磁共振成像(MRI)对儿科 HSCT 患者的区域性肺通气异常进行定量,并与肺活量测定法进行比较。
23 例(年龄 6-16 岁)病情稳定的儿科异基因 HSCT 患者接受了门诊 MRI 扫描,其中使用超极化 Xe 气体进行屏气来定量区域性通气。通气缺陷是指由于阻塞导致通气不良的肺部区域,其通气缺陷百分比(VDP)与肺活量测定法中的 1 秒用力呼气量(FEV)、FEV/用力肺活量(FVC)比值和 25-75%用力肺活量时的用力呼气流量(FEF)进行比较,采用线性回归。
Xe VDP 的平均值±标准差为 10.5±9.4%(范围 2.6-41.4%)。Xe VDP 与 FEV、FEV/FVC 比值和 FEF 相关(所有比较的 p 值均≤0.02)。在 FEV >80%的肺功能正常的患者中也发现了通气缺陷,支持 Xe MRI 对其他肺部疾病中早期阻塞的敏感性。7(30%)例患者无法进行肺活量测定,但其中 5 例患者存在通气缺陷,发现了可能未被发现和未得到治疗的异常,否则这些异常可能会一直未被发现和未得到治疗直到病情进展。
在无症状的儿科 HSCT 患者和无法进行可靠的肺活量测定法的亚组患者中,使用超极化 Xe 气体 MRI 检测到了肺通气缺陷。Xe MRI 为这个可能难以诊断的儿科人群提供了一种可靠的基于成像的肺受累评估方法。