University Clinic for Hematology, Oncology, Hemostaseology and Palliative Care, Johannes Wesling Medical Center Minden, UKRUB, University of Bochum, Hans-Nolte-Straße 1, 32429, Minden, Germany.
Hôpital Saint-Louis, AP-HP, Centre d'Investigations Cliniques (CIC 1427), Université Paris Diderot, INSERM UMRS 1131, 1 Avenue Claude Vellefaux, Paris, France.
Ann Hematol. 2019 May;98(5):1071-1082. doi: 10.1007/s00277-019-03625-x. Epub 2019 Mar 8.
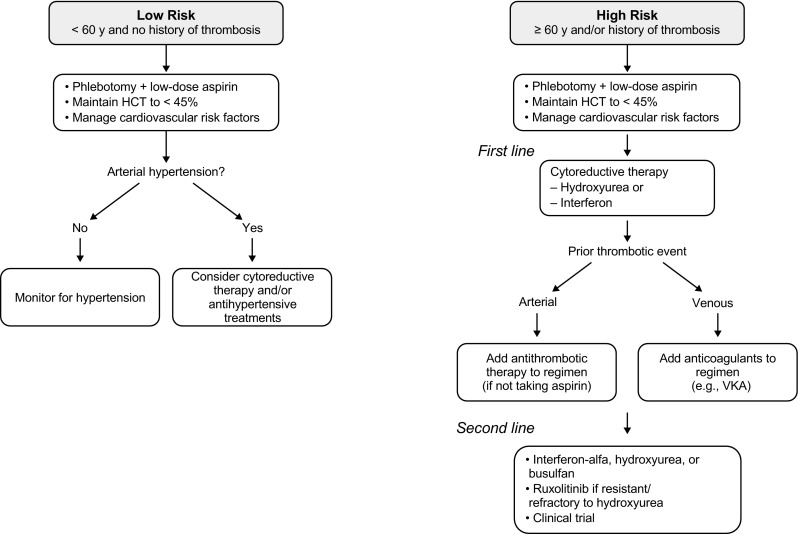
Thromboembolic events and cardiovascular disease are the most prevalent complications in patients with polycythemia vera (PV) compared with other myeloproliferative disorders and are the major cause of morbidity and mortality in this population. Moreover, a vascular complication such as arterial or venous thrombosis often leads to the diagnosis of PV. The highest rates of thrombosis typically occur shortly before or at diagnosis and decrease over time, probably due to the effects of treatment. Important risk factors include age (≥ 60 years old) and a history of thrombosis; elevated hematocrit and leukocytosis are also associated with an increased risk of thrombosis. The goal of therapy is to reduce the risk of thrombosis by controlling hematocrit to < 45%, a target associated with reduced rates of cardiovascular death and major thrombosis. Low-risk patients (< 60 years old with no history of thrombosis) are managed with phlebotomy and low-dose aspirin, whereas high-risk patients (≥ 60 years old and/or with a history of thrombosis) should be treated with cytoreductive agents. Interferon and ruxolitinib are considered second-line therapies for patients who are intolerant of or have an inadequate response to hydroxyurea, which is typically used as first-line therapy. In this review, we discuss factors associated with thrombosis and recent data on current treatments, including anticoagulation, highlighting the need for more controlled studies to determine the most effective cytoreductive therapies for reducing the risk of thrombosis in patients with PV.
血栓栓塞事件和心血管疾病是真性红细胞增多症(PV)患者中最常见的并发症,与其他骨髓增殖性疾病相比,也是该人群发病率和死亡率的主要原因。此外,血管并发症如动脉或静脉血栓通常导致 PV 的诊断。血栓形成的最高发生率通常发生在诊断前或诊断时不久,随着时间的推移而降低,这可能是由于治疗的影响。重要的危险因素包括年龄(≥60 岁)和血栓形成史;血细胞比容和白细胞增多也与血栓形成风险增加相关。治疗的目的是通过将血细胞比容控制在<45%以下来降低血栓形成的风险,这一目标与降低心血管死亡和主要血栓形成的风险相关。低危患者(<60 岁且无血栓形成史)采用放血和低剂量阿司匹林治疗,而高危患者(≥60 岁和/或有血栓形成史)应使用细胞减灭剂治疗。干扰素和芦可替尼被认为是不耐受或对羟基脲反应不足的患者的二线治疗药物,羟基脲通常被用作一线治疗药物。在这篇综述中,我们讨论了与血栓形成相关的因素以及最近关于当前治疗方法的数据,包括抗凝治疗,强调需要更多的对照研究来确定最有效的细胞减灭治疗方法,以降低 PV 患者的血栓形成风险。