Center for Communicable Disease Dynamics, Department of Epidemiology, Harvard TH Chan School of Public Health, Boston, MA 02115 USA.
Center for Communicable Disease Dynamics, Department of Epidemiology, Harvard TH Chan School of Public Health, Boston, MA 02115 USA.
Int J Antimicrob Agents. 2019 Jul;54(1):23-34. doi: 10.1016/j.ijantimicag.2019.03.004. Epub 2019 Mar 6.
Rates of hospitalization with sepsis/septicemia and associated mortality in the US have risen significantly during the last two decades. Antibiotic resistance may contribute to the rates of sepsis-related outcomes through lack of clearance of bacterial infections following antibiotic treatment during different stages of infection. However, there is limited information about the relationship between prevalence of resistance to various antibiotics in different bacteria and rates of sepsis-related outcomes.
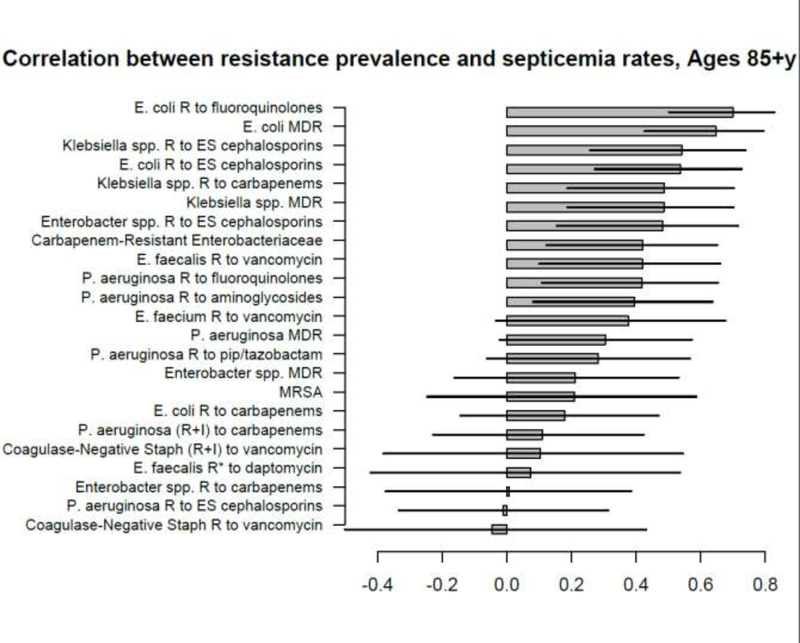
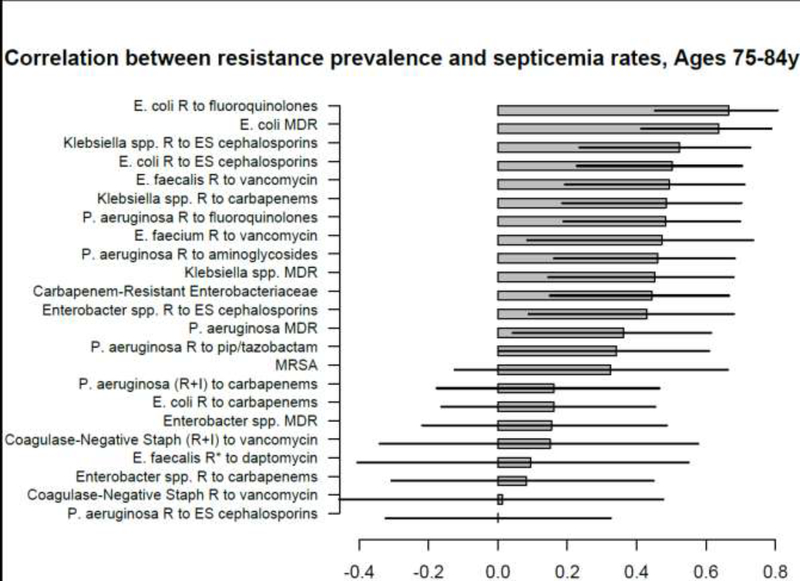
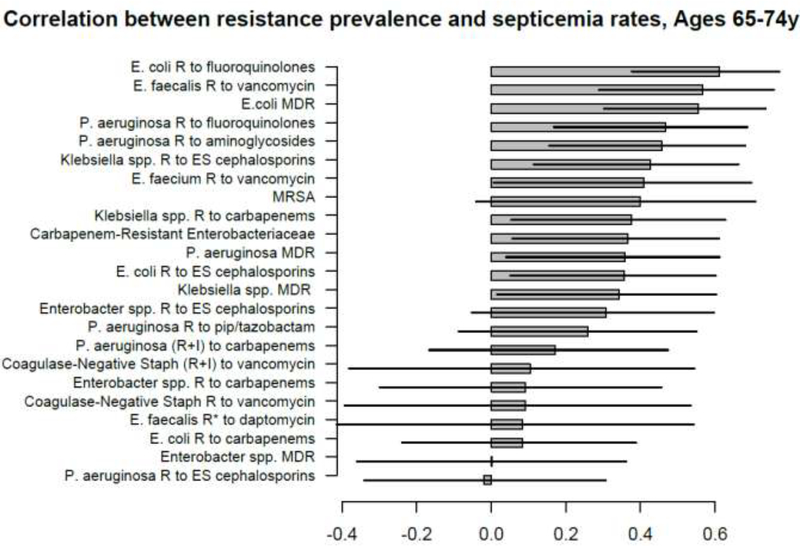
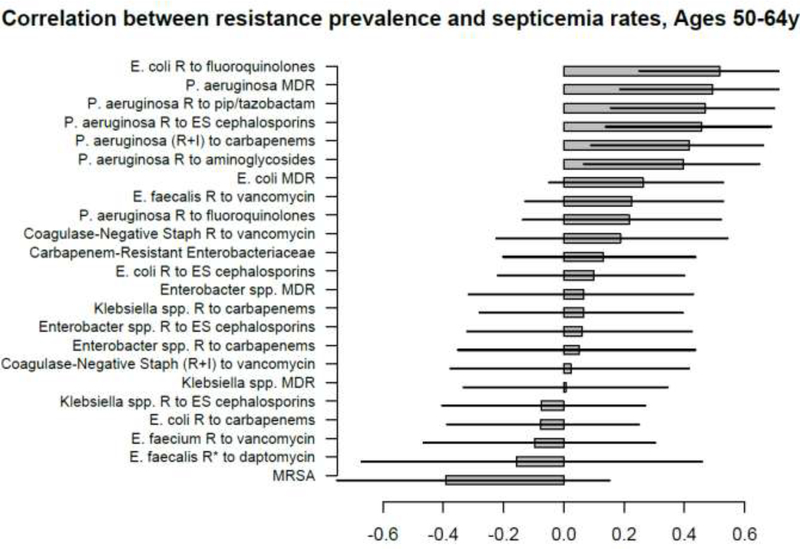
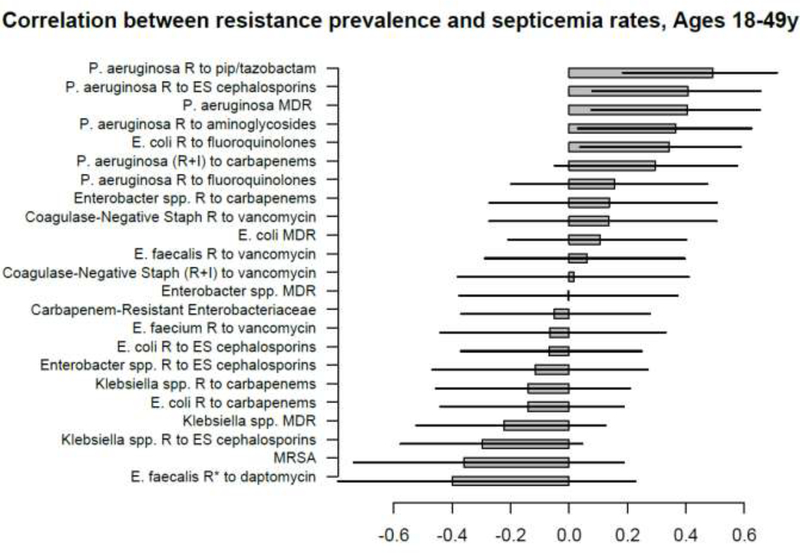
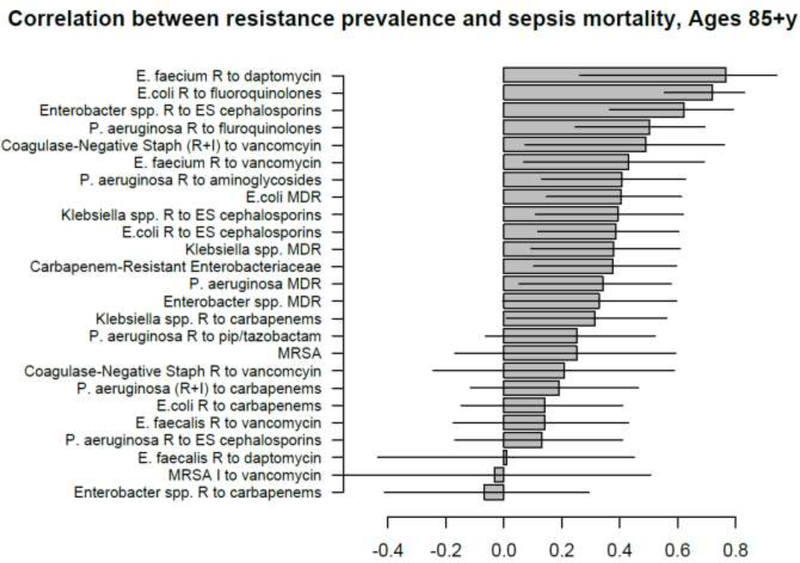
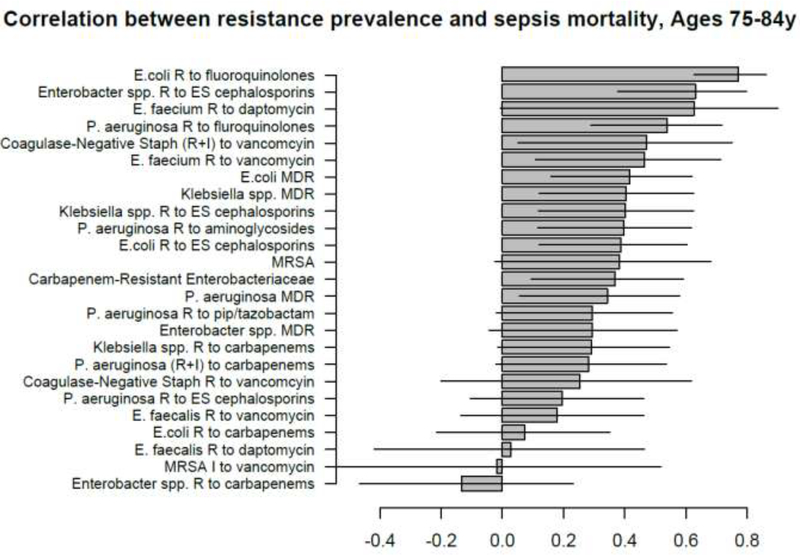
For different age groups of adults (18-49y, 50-64y, 65-74y, 75-84y, 85+y) and combinations of antibiotics/bacteria, we evaluated associations between state-specific prevalence (percentage) of resistant samples for a given combination of antibiotics/bacteria among catheter-associated urinary tract infections (CAUTIs) in the CDC Antibiotic Resistance Patient Safety Atlas data between 2011-2014, and rates of hospitalization with septicemia (ICD-9 codes 038.xx present on the discharge diagnosis) reported to the Healthcare Cost and Utilization Project (HCUP), as well as rates of mortality with sepsis (ICD-10 codes A40-41.xx present on death certificate).
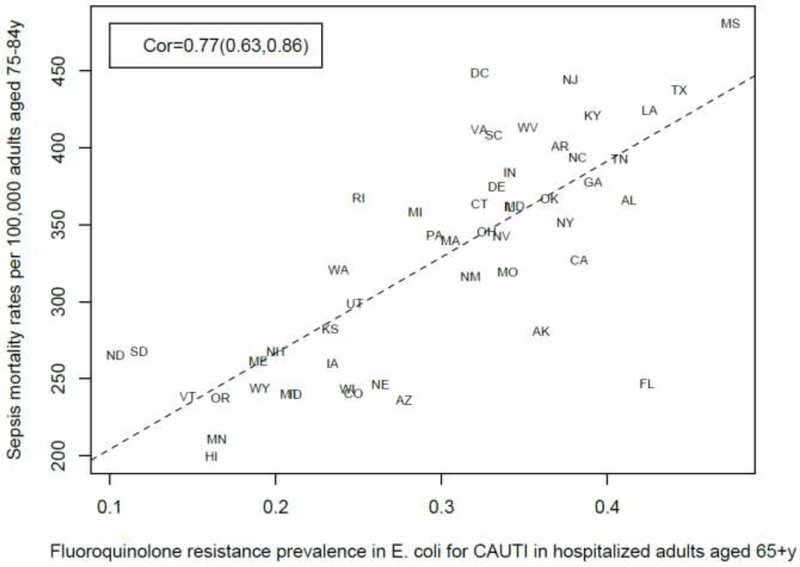
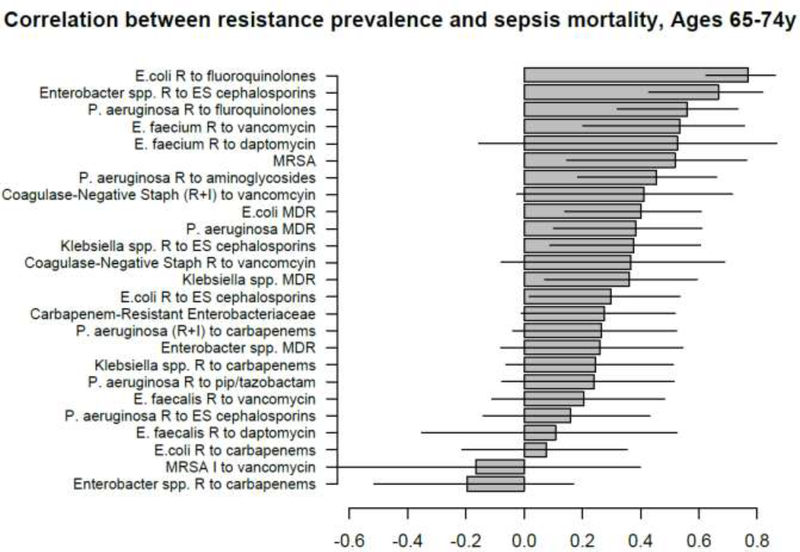
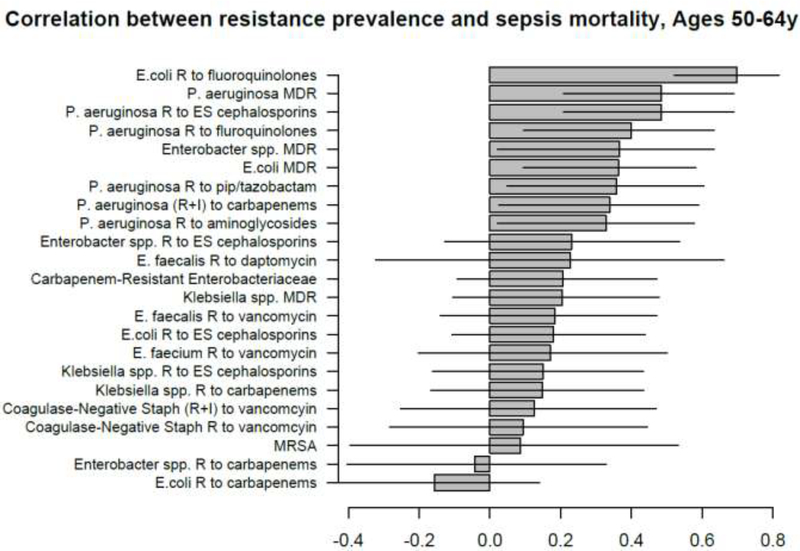
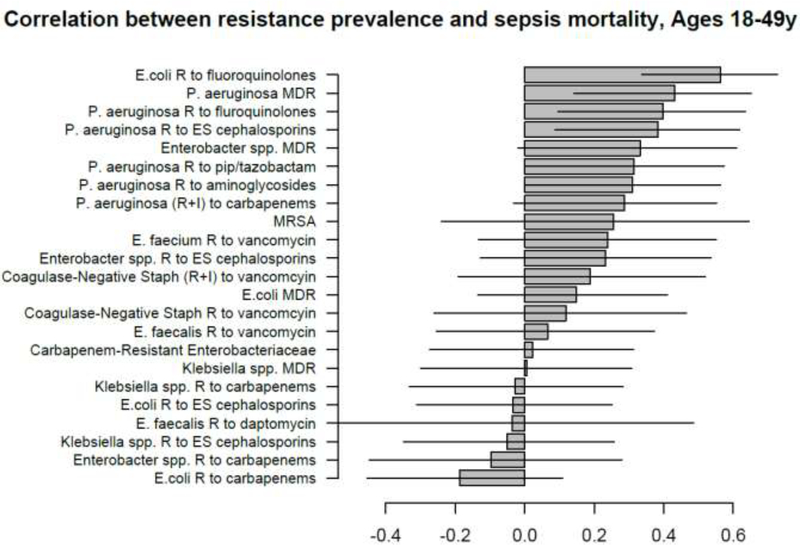
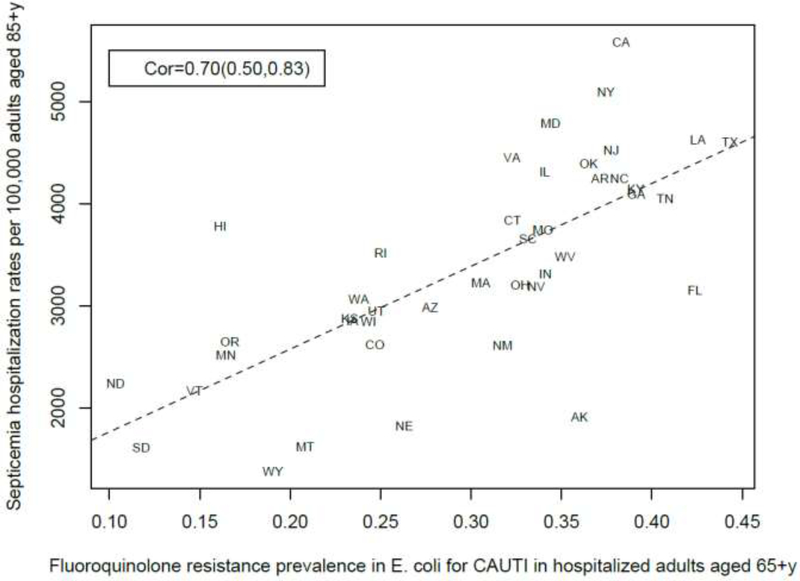
Among the different combinations of antibiotics/bacteria, prevalence of resistance to fluoroquinolones in Escherichia coli had the strongest association with septicemia hospitalization rates for individuals aged over 50y, and with sepsis mortality rates for individuals aged 18-84y. There were several positive correlations between prevalence of resistance for different combinations of antibiotics/bacteria and septicemia hospitalization/sepsis mortality rates in adults.
These findings, and those from work on the relationship between antibiotic use and sepsis rates, support the association between use of/resistance to certain antibiotics and rates of sepsis-related outcomes, indicating the potential utility of antibiotic replacement.
在过去的二十年中,美国因败血症/脓毒症住院的人数和相关死亡率显著上升。抗生素耐药性可能会通过在感染的不同阶段在抗生素治疗后无法清除细菌感染而导致与败血症相关的结局发生率上升。然而,关于不同细菌中各种抗生素耐药率与败血症相关结局发生率之间的关系,相关信息有限。
对于不同年龄组的成年人(18-49 岁、50-64 岁、65-74 岁、75-84 岁、85 岁以上)以及抗生素/细菌的组合,我们评估了 2011-2014 年期间 CDC 抗生素耐药患者安全地图数据中导管相关性尿路感染(CAUTI)中特定州耐药样本的比例(给定抗生素/细菌组合的百分比)与向医疗保健成本和利用项目(HCUP)报告的败血症(ICD-9 代码 038.xx 在出院诊断中)住院率,以及败血症死亡率(死亡证明上 ICD-10 代码 A40-41.xx)之间的关系。
在不同的抗生素/细菌组合中,大肠埃希菌对氟喹诺酮类药物的耐药率与 50 岁以上个体的败血症住院率最强相关,与 18-84 岁个体的败血症死亡率最强相关。不同抗生素/细菌组合的耐药率之间存在几种正相关关系,与成年人的败血症住院/败血症死亡率相关。
这些发现以及抗生素使用与败血症率之间关系的研究结果,支持了某些抗生素的使用/耐药性与败血症相关结局发生率之间的关系,表明抗生素替代的潜在效用。