Department of Internal Medicine, New York University School of Medicine, New York City, New York, USA.
Division of Cardiology, New York University School of Medicine, New York City, New York, USA.
BMJ Open. 2019 Mar 8;9(3):e024548. doi: 10.1136/bmjopen-2018-024548.
To characterise the variation in composition, leadership, and activation criteria of rapid response and cardiac arrest teams in five north-eastern states of the USA.
Cross-sectional study consisting of a voluntary 46-question survey of acute care hospitals in north-eastern USA.
Acute care hospitals in New York, New Jersey, Rhode Island, Vermont, and Pennsylvania.
Surveys were completed by any member of the rapid response team (RRT) with a working knowledge of team composition and function. Participants were all Medicare-participating acute care hospitals, including teaching and community hospitals as well as hospitals from rural, urban and suburban areas.
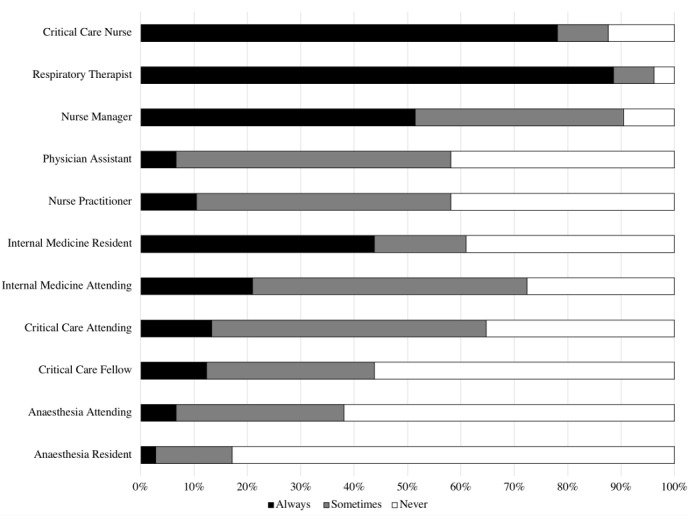
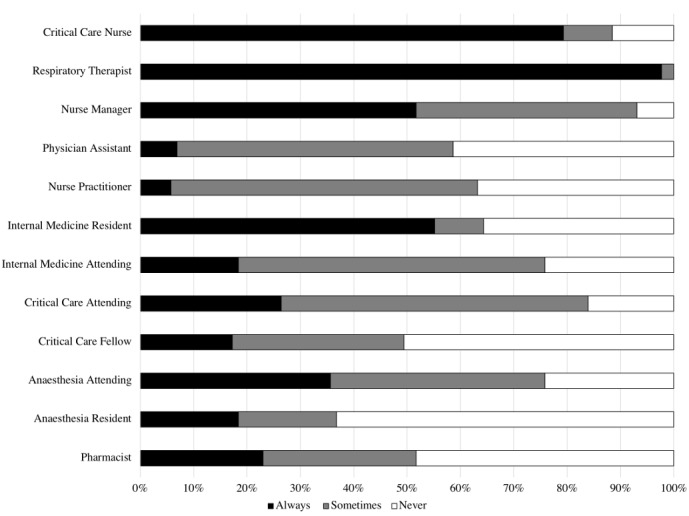
Out of 378 hospitals, contacts were identified for 303, and 107 surveys were completed. All but two hospitals had an RRT, 70% of which changed members daily. The most common activation criteria were clinical concern (95%), single vital sign abnormalities (77%) and early warning score (59%). Eighty one per cent of hospitals had a dedicated cardiac arrest team.RRT composition varied widely, with respiratory therapists, critical care nurses, physicians and nurse managers being the most likely to attend (89%, 78%, 64% and 51%, respectively). Consistent presence of critical care physicians was uncommon and both cardiac arrest teams and teams were frequently led by trainee physicians, often without senior supervision.
As the largest study to date in the USA, we have demonstrated wide heterogeneity, rapid team turnover and a lack of senior supervision of RRT and cardiac arrest teams. These factors likely contribute to the mixed results seen in studies of RRTs.
描述美国东北部五个州的快速反应和心脏骤停团队在组成、领导和激活标准方面的差异。
对美国东北部急性护理医院进行的一项包含 46 个问题的横断面调查。
纽约、新泽西、罗得岛、佛蒙特和宾夕法尼亚的急性护理医院。
对团队组成和功能有一定了解的快速反应团队(RRT)的任何成员均可完成调查。参与者均为参与医疗保险的急性护理医院,包括教学医院和社区医院以及来自农村、城市和郊区的医院。
在 378 家医院中,确定了 303 家医院的联系人,并完成了 107 份调查。除了两家医院外,所有医院都有 RRT,其中 70%的 RRT 每天更换成员。最常见的激活标准是临床关注(95%)、单个生命体征异常(77%)和早期预警评分(59%)。81%的医院有专门的心脏骤停团队。RRT 的组成差异很大,最有可能参加的是呼吸治疗师、重症监护护士、医生和护士长(分别为 89%、78%、64%和 51%)。重症监护医生的持续存在并不常见,心脏骤停团队和 RRT 团队通常由住院医师领导,通常没有高级监督。
作为迄今为止在美国进行的最大规模研究,我们已经证明了快速反应和心脏骤停团队的异质性大、团队人员流动快且缺乏高级监督。这些因素可能是导致 RRT 研究结果不一致的原因。