van Zyl Martin, Witt Chance M, Bhatia Subir, Khasawneh Majd, Gaba Prakriti, Lenz Charles J, Rosenbaum Andrew N, Aung Htin, Hodge David O, McLeod Christopher J, Asirvatham Samuel J
Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, USA.
Department of Internal Medicine, Mayo Clinic, Rochester, MN, USA.
Indian Pacing Electrophysiol J. 2019 Mar-Apr;19(2):40-46. doi: 10.1016/j.ipej.2019.03.001. Epub 2019 Mar 8.
The prognostic significance of paced QRS complex morphology on surface ECG remains unclear. This study aimed to assess long-term outcomes associated with variations in the paced QRS complex.
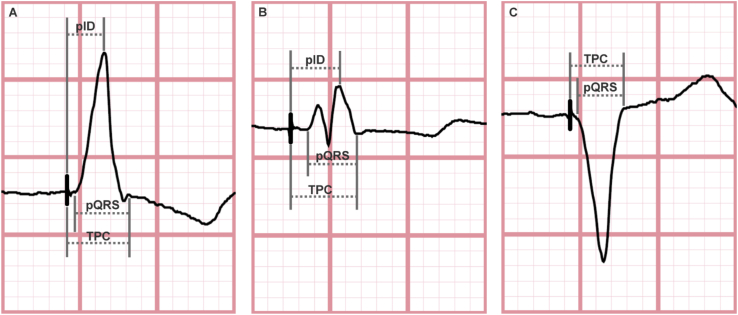
Adult patients who underwent dual-chamber pacemaker implantation with 20% or more ventricular pacing and a 12-lead ECG showing a paced complex were included. The paced QRS was analyzed in leads I and aVL. Long-term clinical and echocardiographic outcomes were compared at 5 years.
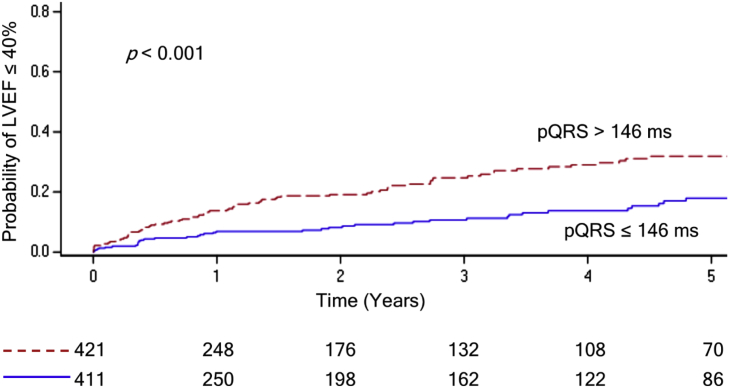
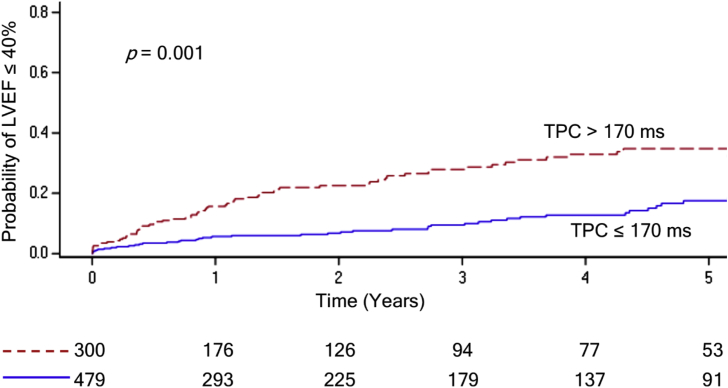
The study included 844 patients (43.1% female; age 75.0 ± 12.1). Patients with a longer paced QRS (pQRS) duration in lead I had a lower rate of atrial fibrillation (HR 0.80; p = 0.03) and higher rate of systolic dysfunction (HR 1.17; p < 0.001). Total pacing complex (TPC) duration was linked to higher rates of ICD implantation (HR 1.18; p = 0.04) and systolic dysfunction (HR 1.22, p < 0.001). Longer paced intrinsicoid deflection (pID) was associated with less atrial fibrillation (HR 0.75; p = 0.01), more systolic dysfunction (HR 1.17; p < 0.001), ICD implantation (HR 1.23; p = 0.04), and CRT upgrade (HR 1.23; p = 0.03). Exceeding thresholds for TPC, pQRS, and pID of 170, 146, and 112 ms in lead I, respectively, was associated with a substantial increase in systolic dysfunction over 5 years (p < 0.001).
Longer durations of all tested parameters in lead I were associated with increased rates of left ventricular systolic dysfunction. ICD implantation and CRT upgrade were also linked to increased TPC and pID durations. Paradoxically, patients with longer pID and pQRS had less incident atrial fibrillation.
体表心电图上起搏QRS波群形态的预后意义仍不明确。本研究旨在评估与起搏QRS波群变化相关的长期预后。
纳入接受双腔起搏器植入且心室起搏比例达20%或更高、12导联心电图显示有起搏波群的成年患者。对I导联和aVL导联的起搏QRS波群进行分析。比较5年时的长期临床和超声心动图预后。
该研究纳入了844例患者(女性占43.1%;年龄75.0±12.1岁)。I导联起搏QRS波群(pQRS)时限较长的患者房颤发生率较低(HR 0.80;p = 0.03),收缩功能障碍发生率较高(HR 1.17;p < 0.001)。总起搏波群(TPC)时限与更高的植入式心律转复除颤器(ICD)植入率(HR 1.18;p = 0.04)和收缩功能障碍发生率(HR 1.22,p < 0.001)相关。起搏固有波峰时限(pID)较长与较少的房颤(HR 0.75;p = 0.01)、较多的收缩功能障碍(HR 1.17;p < 0.001)、ICD植入(HR 1.23;p = 0.04)以及心脏再同步治疗升级(HR 1.23;p = 0.03)相关。I导联中TPC、pQRS和pID分别超过170、146和112毫秒的阈值与5年内收缩功能障碍的大幅增加相关(p < 0.001)。
I导联中所有测试参数的较长时限与左心室收缩功能障碍发生率增加相关。ICD植入和心脏再同步治疗升级也与TPC和pID时限增加相关。矛盾的是,pID和pQRS较长的患者房颤发生率较低。