Shahab Omer, Sayiner Mehmet, Paik James, Felix Sean, Golabi Pegah, Younossi Zobair M
Center for Liver Disease, Department of Medicine Inova Fairfax Hospital Falls Church VA.
Betty and Guy Beatty Center for Integrated Research Inova Health System Falls Church VA.
Hepatol Commun. 2019 Jan 28;3(3):356-364. doi: 10.1002/hep4.1314. eCollection 2019 Mar.
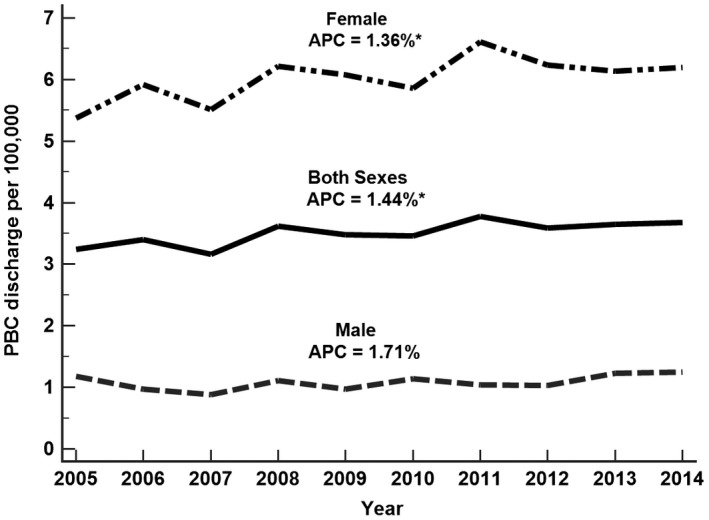
Primary biliary cholangitis (PBC) is an autoimmune liver disease that can lead to cirrhosis and liver failure. Our aim was to assess the recent trends in the mortality rates and health care utilization of patients with PBC seen in the inpatient setting in the United States. We used the National (Nationwide) Inpatient Sample data (2005-2014). The study population included adults with PBC, using International Classification of Diseases, Ninth Revision codes. Trends in PBC-related discharges, total charges, length of stay (LoS), and in-hospital mortality were evaluated. Hierarchical generalized linear models were performed for determining predictors of mortality and total hospital charges. Between the study years of 2005 and 2014, a total of 22,665 hospitalized cases with PBC were identified (mean age 63 years; 84% female, 76% white). The number of PBC-related discharges increased from 3.24 per 100,000 in 2005 to 3.68 per 100,000 in 2014, with an average annual increase of 1.4% (95% confidence interval [CI]: 0.4%-2.4%). Fifty-seven percent had Medicare as their primary payer, 37% had cirrhosis, and 1.3% had hepatocellular carcinoma. Between 2005 and 2014, the average total charges for PBC increased from $53,901 to $57,613 (annual percent change [APC], 1.7%; 95% CI: -0.2%-3.5%), LoS decreased from 6.9 days to 5.4 days (APC, -2.2%; 95% CI: -3.2% to -1.1%), and mortality rate decreased from 3.8% to 2.8% (APC, -5.4%; 95% CI: -8.4% to -2.4%). Multivariable analysis revealed that ascites were independently associated with increased risk of in-hospital mortality (odds ratio: 1.77; 95% CI: 1.50-2.08), increased charge (percent change: 22.5%; 95% CI: 18.6%-26.7%), and increased LoS (percent change: 29.7%; 95% CI: 25.7%-33.9%). The number of PBC cases has increased in recent years. Mortality and LoS have decreased, and the total charges have remained the same.
原发性胆汁性胆管炎(PBC)是一种自身免疫性肝病,可导致肝硬化和肝衰竭。我们的目的是评估美国住院患者中PBC患者的死亡率和医疗保健利用率的近期趋势。我们使用了全国住院患者样本数据(2005 - 2014年)。研究人群包括患有PBC的成年人,采用国际疾病分类第九版编码。评估了与PBC相关的出院人数、总费用、住院时间(LoS)和住院死亡率的趋势。进行了分层广义线性模型以确定死亡率和医院总费用的预测因素。在2005年至2014年的研究期间,共识别出22,665例住院的PBC病例(平均年龄63岁;84%为女性,76%为白人)。与PBC相关的出院人数从2005年的每10万人3.24例增加到2014年的每10万人3.68例,平均每年增加1.4%(95%置信区间[CI]:0.4% - 2.4%)。57%的患者以医疗保险作为主要支付方,37%的患者患有肝硬化,1.3%的患者患有肝细胞癌。在2005年至2014年期间,PBC的平均总费用从53,901美元增加到57,613美元(年百分比变化[APC],1.7%;95% CI: - 0.2% - 3.5%),住院时间从6.9天降至5.4天(APC, - 2.2%;95% CI: - 3.2%至 - 1.1%),死亡率从3.8%降至2.8%(APC, - 5.4%;95% CI: - 8.4%至 - 2.4%)。多变量分析显示,腹水与住院死亡率增加风险独立相关(比值比:1.77;95% CI:1.50 - 2.08)、费用增加(百分比变化:22.5%;95% CI:18.6% - 26.7%)和住院时间增加(百分比变化:29.7%;95% CI:25.7% - 33.9%)。近年来,PBC病例数有所增加。死亡率和住院时间有所下降,总费用保持不变。