1 Dana-Farber Cancer Institute, Boston, MA.
2 University of North Carolina at Chapel Hill, Chapel Hill, NC.
J Clin Oncol. 2019 May 1;37(13):1081-1089. doi: 10.1200/JCO.18.01511. Epub 2019 Mar 12.
Evidence-based treatments for metastatic, human epidermal growth factor receptor 2 (HER2)-positive breast cancer to the CNS are limited. We previously reported modest activity of neratinib monotherapy for HER2-positive breast cancer brain metastases. Here we report the results from additional study cohorts.
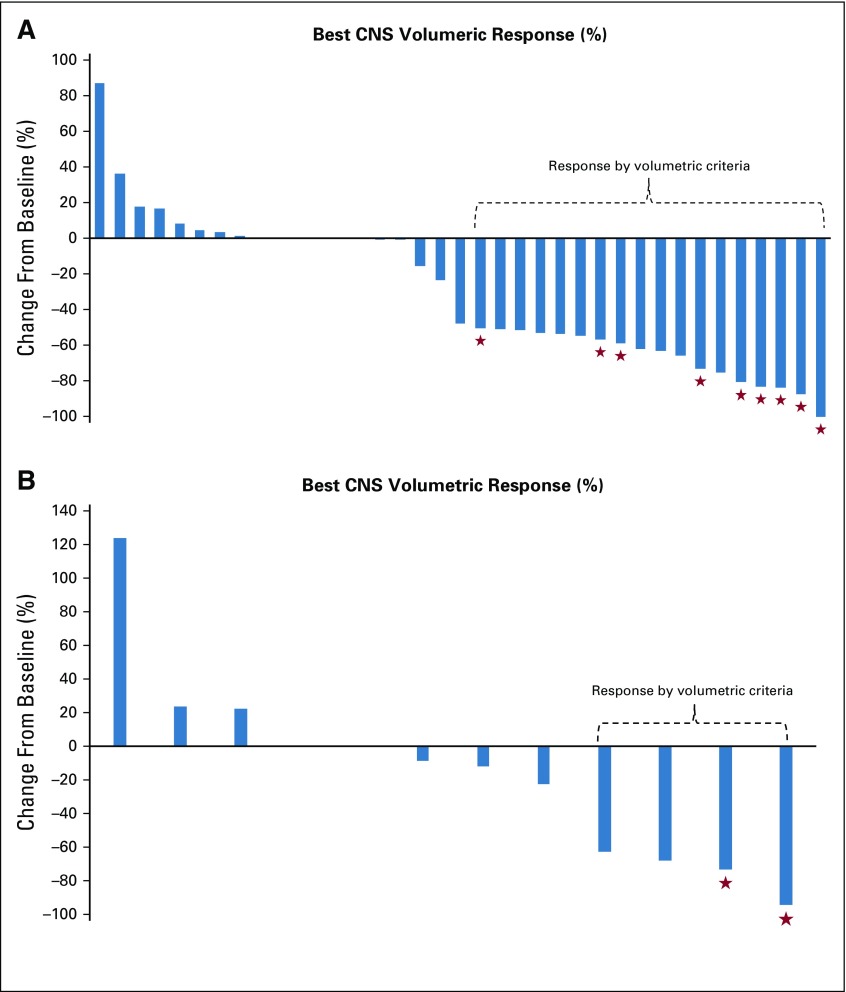
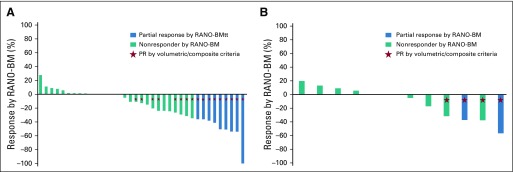
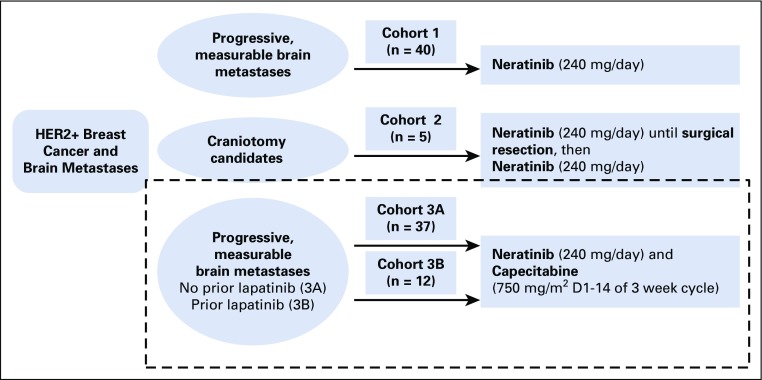
Patients with measurable, progressive, HER2-positive brain metastases (92% after receiving CNS surgery and/or radiotherapy) received neratinib 240 mg orally once per day plus capecitabine 750 mg/m twice per day for 14 days, then 7 days off. Lapatinib-naïve (cohort 3A) and lapatinib-treated (cohort 3B) patients were enrolled. If nine or more of 35 (cohort 3A) or three or more of 25 (cohort 3B) had CNS objective response rates (ORR), the drug combination would be deemed promising. The primary end point was composite CNS ORR in each cohort separately, requiring a reduction of 50% or more in the sum of target CNS lesion volumes without progression of nontarget lesions, new lesions, escalating steroids, progressive neurologic signs or symptoms, or non-CNS progression.
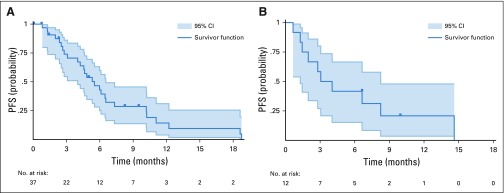
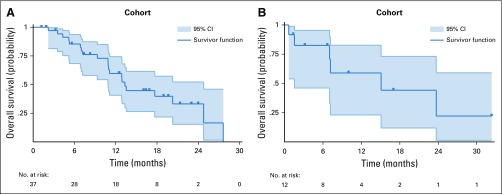
Forty-nine patients enrolled in cohorts 3A (n = 37) and 3B (n = 12; cohort closed for slow accrual). In cohort 3A, the composite CNS ORR = 49% (95% CI, 32% to 66%), and the CNS ORR in cohort 3B = 33% (95% CI, 10% to 65%). Median progression-free survival was 5.5 and 3.1 months in cohorts 3A and 3B, respectively; median survival was 13.3 and 15.1 months. Diarrhea was the most common grade 3 toxicity (29% in cohorts 3A and 3B).
Neratinib plus capecitabine is active against refractory, HER2-positive breast cancer brain metastases, adding additional evidence that the efficacy of HER2-directed therapy in the brain is enhanced by chemotherapy. For optimal tolerance, efforts to minimize diarrhea are warranted.
针对转移性人表皮生长因子受体 2(HER2)阳性乳腺癌脑转移的循证治疗方法有限。我们之前报道过奈拉替尼单药治疗 HER2 阳性乳腺癌脑转移的适度疗效。在此,我们报告了额外研究队列的结果。
有可测量的、进展性的 HER2 阳性脑转移(92%的患者在接受 CNS 手术后和/或放射治疗后)的患者接受口服奈拉替尼 240mg 每日一次加卡培他滨 750mg/m2 每日两次,连用 14 天,然后停药 7 天。纳拉替尼初治(队列 3A)和纳拉替尼治疗(队列 3B)的患者被纳入。如果 35 例患者中有 9 例或以上(队列 3A)或 25 例患者中有 3 例或以上(队列 3B)有中枢神经系统客观缓解率(ORR),则认为该药物联合具有前景。主要终点是每个队列的复合 CNS ORR,要求目标 CNS 病变体积总和减少 50%或更多,且非目标病变、新病变、递增类固醇、进行性神经体征或症状或非 CNS 进展无进展。
49 例患者入组队列 3A(n=37)和 3B(n=12;因入组缓慢而关闭队列)。在队列 3A 中,复合 CNS ORR=49%(95%CI,32%至 66%),队列 3B 的 CNS ORR=33%(95%CI,10%至 65%)。队列 3A 和 3B 的中位无进展生存期分别为 5.5 个月和 3.1 个月;中位生存期分别为 13.3 个月和 15.1 个月。腹泻是最常见的 3 级毒性(队列 3A 和 3B 中均为 29%)。
奈拉替尼联合卡培他滨对难治性 HER2 阳性乳腺癌脑转移有效,进一步证明了 HER2 靶向治疗在大脑中的疗效通过化疗增强。为了获得最佳耐受性,有必要努力减少腹泻。