Hočevar Keli, Ristić Smiljana, Peterlin Borut
Clinical Institute of Medical Genetics, University Medical Centre Ljubljana, Ljubljana, Slovenia.
Department of Biology and Medical Genetics, School of Medicine, University of Rijeka, Rijeka, Croatia.
Front Neurol. 2019 Feb 26;10:134. doi: 10.3389/fneur.2019.00134. eCollection 2019.
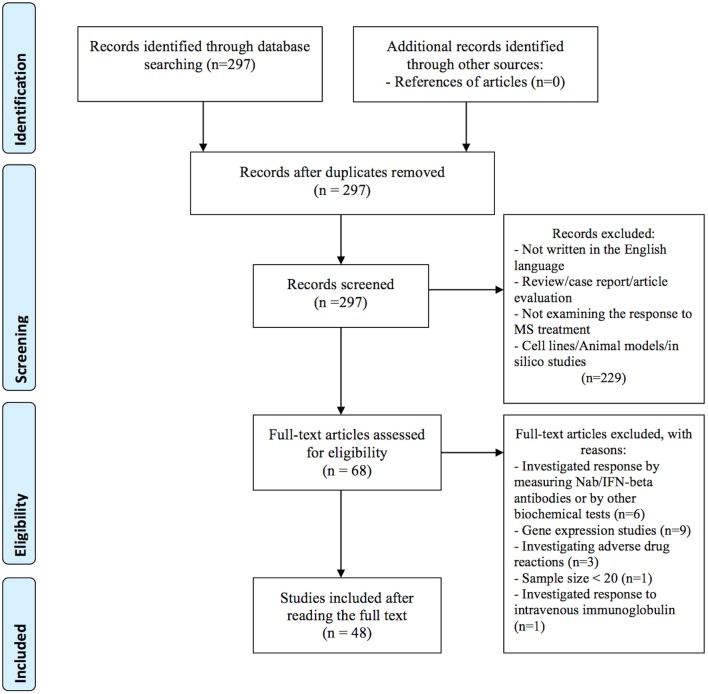
Over the past two decades, various novel disease-modifying drugs for multiple sclerosis (MS) have been approved. However, there is high variability in the patient response to the available medications, which is hypothesized to be partly attributed to genetics. To conduct a systematic review of the current literature on the pharmacogenomics of MS therapy. A systematic literature search was conducted using PubMed/MEDLINE database searching for articles investigating a role of genetic variation in response to disease-modifying MS treatments, published in the English language up to October 9th, 2018. PRISMA guidelines for systematic reviews were applied. Studies were included if they investigated response or nonresponse to MS treatment defined as relapse rate, by expanded disability status scale score or based on magnetic resonance imaging. The following data were extracted: first author's last name, year of publication, PMID number, sample size, ethnicity of patients, method, genes, and polymorphisms tested, outcome, significant associations with corresponding -values and confidence intervals, response criteria, and duration of the follow-up period. Overall, 48 articles published up to October 2018, evaluating response to interferon-beta, glatiramer acetate, mitoxantrone, and natalizumab, met our inclusion criteria and were included in this review. Among those, we identified 42 (87.5%) candidate gene studies and 6 (12.5%) genome-wide association studies. Existing pharmacogenomic evidence is mainly based on the results of individual studies, or on results of multiple studies, which often lack consistency. In recent years, hypothesis-free approaches identified novel candidate genes that remain to be validated. Various study designs, including the definition of clinical response, duration of the follow-up period, and methodology as well as moderate sample sizes, likely contributed to discordances between studies. However, some of the significant associations were identified in the same genes, or in the genes involved in the same biological pathways. At the moment, there is no available clinically actionable pharmacogenomic biomarker that would enable more personalized treatment of MS. More large-scale studies with uniform design are needed to identify novel and validate existing pharmacogenomics findings. Furthermore, studies investigating associations between rare variants and treatment response in MS patients, using next-generation sequencing technologies are warranted.
在过去二十年中,多种用于治疗多发性硬化症(MS)的新型疾病修正药物已获批准。然而,患者对现有药物的反应存在很大差异,据推测部分原因是遗传因素。为了对当前关于MS治疗药物基因组学的文献进行系统综述。使用PubMed/MEDLINE数据库进行了系统的文献检索,以查找研究基因变异在对MS疾病修正治疗反应中作用的文章,这些文章截至2018年10月9日以英文发表。应用了系统综述的PRISMA指南。如果研究调查了对MS治疗的反应或无反应,将其定义为复发率、扩展残疾状态量表评分或基于磁共振成像,则纳入研究。提取了以下数据:第一作者姓氏、发表年份、PMID编号、样本量、患者种族、方法、测试的基因和多态性、结果、与相应P值和置信区间的显著关联、反应标准以及随访期时长。总体而言,截至2018年10月发表的48篇评估对干扰素-β、醋酸格拉替雷、米托蒽醌和那他珠单抗反应的文章符合我们的纳入标准,并被纳入本综述。其中,我们确定了42项(87.5%)候选基因研究和6项(12.5%)全基因组关联研究。现有的药物基因组学证据主要基于个别研究的结果,或基于多个研究的结果,而这些结果往往缺乏一致性。近年来,无假设方法确定了有待验证的新型候选基因。各种研究设计,包括临床反应的定义、随访期时长、方法以及中等样本量,可能导致了研究之间的不一致。然而,一些显著关联在相同基因或参与相同生物学途径的基因中被发现。目前,尚无可用的临床可行药物基因组学生物标志物能够实现MS更个性化的治疗。需要更多设计统一的大规模研究来识别新的药物基因组学发现并验证现有发现。此外,有必要开展研究,利用下一代测序技术调查MS患者中罕见变异与治疗反应之间的关联。