1 Department of Cardiology, Erasmus MC, University Medical Center Rotterdam, The Netherlands.
2 Department of Cardiology, Maastricht University Medical Center, The Netherlands.
Eur J Prev Cardiol. 2019 Sep;26(13):1399-1407. doi: 10.1177/2047487319835042. Epub 2019 Mar 13.
Elderly patients are underrepresented in clinical trials but comprise the majority of heart failure patients. Data on age-specific use of heart failure therapy are limited. The European Society of Cardiology heart failure guidelines provide no age-specific treatment recommendations. We investigated practice-based heart failure management in a large registry at heart failure outpatient clinics.
We studied 8351 heart failure with reduced ejection fraction patients at 34 Dutch outpatient clinics between 2013 and 2016. The mean age was 72.3 ± 11.8 years and we divided age into three categories: less than 60 years (13.9%); 60-74 years (36.0%); and 75 years and over (50.2%).
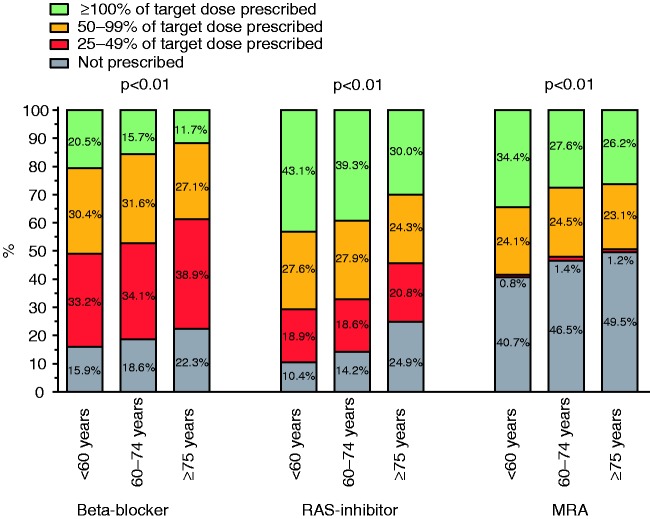
Elderly heart failure with reduced ejection fraction patients (≥75 years) received significantly fewer beta-blockers (77.8% vs. 84.2%), renin-angiotensin system inhibitors (75.2% vs. 89.7%), mineralocorticoid receptor antagonists (50.6% vs. 59.6%) and ivabradine (2.9% vs. 9.3%), but significantly more diuretics (88.1% vs. 72.6%) compared to patients aged less than 60 years ( < 0.01). Moreover, the prescribed target dosages were significantly lower in elderly patients. Also, implantable cardioverter defibrillator (18.9% vs. 44.1%) and cardiac resynchronisation therapy device (14.6% vs. 16.7%) implantation rates were significantly lower in elderly patients. A similar trend in drug prescription was observed in patients with heart failure with mid-range ejection fraction as in heart failure with reduced ejection fraction.
With increasing age, heart failure with reduced ejection fraction patients less often received guideline-recommended medication prescriptions and also in a lower dosage. In addition, a lower percentage of implantable cardioverter defibrillator and cardiac resynchronisation therapy device implantation in elderly patients was observed.
临床试验中老年人代表性不足,但占心力衰竭患者的大多数。关于心力衰竭治疗的特定年龄数据有限。欧洲心脏病学会心力衰竭指南没有提供特定年龄的治疗建议。我们在心力衰竭门诊诊所的大型注册中心调查了基于实践的心力衰竭管理情况。
我们研究了 2013 年至 2016 年间 34 家荷兰门诊诊所的 8351 名射血分数降低的心力衰竭患者。平均年龄为 72.3±11.8 岁,我们将年龄分为三组:小于 60 岁(13.9%);60-74 岁(36.0%);和 75 岁及以上(50.2%)。
年龄较大的射血分数降低的心力衰竭患者(≥75 岁)接受β受体阻滞剂(77.8%对 84.2%)、肾素-血管紧张素系统抑制剂(75.2%对 89.7%)、盐皮质激素受体拮抗剂(50.6%对 59.6%)和伊伐布雷定(2.9%对 9.3%)的比例明显较低,但利尿剂的比例明显较高(88.1%对 72.6%),与年龄小于 60 岁的患者相比(<0.01)。此外,老年患者的处方目标剂量明显较低。同样,在老年患者中,植入式心脏复律除颤器(18.9%对 44.1%)和心脏再同步治疗装置(14.6%对 16.7%)的植入率也明显较低。在射血分数中等的心力衰竭患者中也观察到了类似的药物处方趋势。
随着年龄的增长,射血分数降低的心力衰竭患者接受指南推荐的药物处方的比例较低,剂量也较低。此外,在老年患者中观察到植入式心脏复律除颤器和心脏再同步治疗装置的植入比例较低。